- Published by:
- Family Safety Victoria
- Date:
- 2 Dec 2019
The Victorian Government proudly acknowledges Aboriginal and Torres Strait Islander people as the first peoples and Traditional Owners and custodians of the land. We pay respect to Elders, past and present, and acknowledge the ongoing leadership role of the Aboriginal community in addressing and preventing family violence. We would like to acknowledge and thank all stakeholders for their time and their ideas which have contributed to the development of the Victorian Family Violence Data Collection Framework.
Unless indicated otherwise, content in this publication is provided under a Creative Commons Attribution 4.0 International Licence. To view a copy of this licence, visit creativecommons.org/licenses/by/4.0/. It is a condition of the Creative Commons Attribution 4.0 Licence that you must give credit to the original author who is the State of Victoria.
Data Item Reference Guide
Lists each data item in the framework and which section it can be found in.
The table below lists each data item in the framework and the section it can be found in.
| Section | Data item |
|---|---|
| General data items | Names |
| General data items | Age and date of birth |
| General data items | Date variables |
| General data items | Geographic variables (including person address and organisation address) |
| General data items | Unique identifiers |
| General data items | Data linkage |
| Family violence data items | Types of family violence |
| Family violence data items | Relationship between parties |
| Family violence data items | Role of party |
| LGBTI communities | Gender identity |
| LGBTI communities | Sex |
| LGBTI communities | Sexual orientation |
| LGBTI communities | Intersex |
| People with disabilities | Standardised disability flag |
| People with disabilities | Abridged disability set (difficulty experienced, assistance needs) |
| People with disabilities | Disability group |
| People with disabilities | Reasonable adjustments |
| CALD communities | Country of birth |
| CALD communities | Cultural background and ethnicity |
| CALD communities | Main language spoken at home |
| CALD communities | Interpreter required |
| Aboriginal and Torres Strait Islander communities | Standard Indigenous Question |
Acronyms and terminology
Lists acronyms and terminology used throughout this publication.
Acronyms
ABS: Australian Bureau of Statistics
ACCO: Aboriginal Community Controlled Organisation
AFM: Affected family member
AFVITH: Adolescent family violence in the home
AIFS: Australian Institute of Family Studies
AIHW: Australian Institute of Health and Welfare
ANROWS: Australia’s National Research Organisation for Women’s Safety
ASCCEG: Australian Standard Classification of Cultural and Ethnic Groups
ASCL: Australian Standard Classification of Languages
CALD: Culturally and linguistically diverse
CSA: Crime Statistics Agency
CVS: Crime Victimisation Survey
DCRF: Foundation for a National Data Collection and Reporting Framework for family, domestic and sexual violence
DHHS: Department of Health and Human Services
DPC: Department of Premier and Cabinet
EHRC: Equality and Human Rights Commission UK
FVDB: Victorian Family Violence Database
FVPA: Family Violence Protection Act 2008 (Vic)
HPP: Health Privacy Principles
HRA: Health Records Act 2001 (Vic)
IPP: Information Privacy Principles
IRIS: Integrated Reports and Information System
L17: Victoria Police Family Violence Risk Assessment and Management form
LEAP: Victoria Police Law Enforcement Assistance Program
LGBTI: Lesbian, gay, bisexual, transgender and intersex
METeOR: Metadata Online Registry
NATSISS: National Aboriginal and Torres Strait Islander Social Survey
NCIS: National Coronial Information System
NDIS: National Disability Insurance Scheme
NHS: National Health Service England
NTV: No to Violence
ONS: Office for National Statistics UK
PDPA: Privacy and Data Protection Act 2014 (Vic)
PSS: Personal Safety Survey
RCFV: Royal Commission into Family Violence
SACC: Standard Australian Classification of Countries
SDAC: Survey of Disability, Ageing and Carers
SDS: Supplementary Disability Survey
SIQ: Standard Indigenous Question
SLK: Statistical linkage key
UID: Unique identifier
VEOHRC: Victorian Equal Opportunity and Human Rights Commission
VPDSF: Victorian Protective Data Security Framework
Terminology
A glossary appears at the end of each priority community section of this framework which includes definitions specific to each particular section. However, broader terminology which is used throughout the framework is discussed here and is based on language used by the Royal Commission into Family Violence (RCFV).1
Family violence
‘Family violence’ is the term used throughout this framework to refer to a wide range of behaviours identified in the Family Violence Protection Act 2008 (Vic). Information regarding the definition of family violence can be found on page 26. Where this framework directly references materials which use other terms such as ‘domestic violence’ or ‘intimate partner violence’, these terms have been retained, however the scope of these terms is typically more narrow than family violence. Domestic violence may be used to refer to acts of violence between intimate partners and violence in the context of family relationships. It may be used in legislation in other jurisdictions and in practice guidance in some parts of Victoria. Intimate partner violence is commonly used to highlight the predominant manifestation of the violence, which is in the context of current or former intimate partner relationships.
Language about victims
State and national policy and non-government services primarily use the terms ‘victim’, ‘victimsurvivor’ to refer to adults and children who have experienced family violence, as well as ‘woman and their children who experience violence’. The Family Violence Information Sharing Scheme under Part 5A of the Family Violence Protection Act 2008 (Vic) uses the term ‘primary person’ to describe a person about whom there is a reasonable belief there is a risk they may be subjected to family violence. Victoria Police use the term ‘affected family member’ in the context of police attended or reported family violence incidents. In the context of intervention order applications, courts also use the term ‘affected family member’, and use ‘applicant’ to describe the person applying for an order. ‘Victim’ is sometimes considered problematic because it suggests that people who have experienced family violence are helpless or lack the capacity to make rational choices about how to respond to the violence. For the purposes of the framework, the terms ‘victim’, ‘victim-survivor’ and ‘people who experience violence’ (or ‘people who experience abuse’) are used interchangeably, unless referencing material which uses other terms, or specifically discussing information within the context of Victoria Police or courts.
Language about perpetrators
A broad range of terminology is used in relation to people who use violence, including ‘perpetrators’ and ‘men who use violence’. The Family Violence Information Sharing Scheme under Part 5A of the Family Violence Protection Act 2008 (Vic) uses the term ‘person of concern’ to describe a person that there is a reasonable belief there is a risk they may commit family violence. Victoria Police use the term ‘respondent’ to refer to a person described as using violence in the context of police attended or reported family violence incidents. The word ‘defendant’ may be used to describe a person being prosecuted for a family violence offence, and the word ‘offender’ may be used to describe a person who has been found guilty of such an offence. For the purposes of the framework, the terms ‘people who use violence’ and ‘perpetrator’ are used interchangeably.
Priority communities
The communities identified by the RCFV (in recommendation 204) and through consultation are described in the framework as ‘priority communities’. They are: Aboriginal and Torres Strait Islander communities, lesbian, gay, bisexual, transgender and intersex (LGBTI) communities, people with disabilities, culturally and linguistically diverse (CALD) communities, children and young people, and older people.
Administrative data
Administrative data refers to data typically collected by an agency or service provider as a by-product of providing services to clients or otherwise undertaking a core business activity
Mainstream services
Mainstream services in the context of this framework refers to any organisation which provides a service that is not primarily intended to identify or respond to family violence. Such services include police, education facilities, courts and healthcare services.
1 Royal Commission into Family Violence (RCFV) 2016, Volume 1 Report and recommendations, Victoria, p.9.
Introduction
During the RCFV, a number of common data gaps were identified in the current family violence evidence base.
Introduction
During the RCFV, a number of common data gaps were identified in the current family violence evidence base. It was noted that there is a lack of available data to support critical decision making, policy development, planning, research and evaluation activities. The report published by the RCFV outlined gaps in knowledge regarding:
- the demographic characteristics of priority communities, in particular, lesbian, gay, bisexual, transgender and intersex (LGBTI) communities, people with disabilities, Aboriginal and Torres Strait Islander communities, culturally and linguistically diverse (CALD) communities, and older people
- the number of unique clients and the extent to which individuals have multiple engagements with agencies and services related to family violence over time
- a person’s interactions with the system, which is based on the ability to link individuals across different data sets
- the extent of family violence beyond heterosexual intimate partner violence
Addressing the RCFV recommendations
The Crime Statistics Agency (CSA) was commissioned by the Department of Premier and Cabinet (DPC) to address a number of RCFV recommendations related to the collection and reporting of family violence data. The Victorian Family Violence Data Collection Framework (the framework) addresses aspects of three of these recommendations, with the relevant content of these summarised below.
This framework was been developed in consultation with a range of stakeholders, listed at page 109, and with significant input from Family Safety Victoria (FSV).
Recommendation 204 – Improve state-wide family violence data collection and research
Improvements to be made to state-wide family violence data collection and research, through developing a state-wide data framework, informed by relevant Commonwealth standards – for example, relevant Australian Bureau of Statistics (ABS) frameworks such as the National Data Collection and Reporting Framework (DCRF) guidelines and Australia’s National Research Organisation for Women’s Safety (ANROWS) guidance. The framework should include guidelines on the collection of demographic information – in particular, on older people, people with disabilities and people from Aboriginal and Torres Strait Islander, culturally and linguistically diverse and lesbian, gay, bisexual, transgender and intersex communities.
Recommendation 152 – Improve the collection of Indigenous data relating to family violence
Improve the collection of Indigenous-specific data relating to family violence so that this can be shared with communities, organisations and governance forums to inform local, regional and statewide responses.
Recommendation 170 – Adopt a consistent and comprehensive approach to data collection on people with disabilities
The Victorian Government will adopt a consistent and comprehensive approach to the collection of data on people with disabilities who experience or perpetrate family violence.
What is the framework?
The framework is a tool for government and non-government service providers and agencies who collect administrative data in the context of family violence. The framework will help service providers and agencies standardise the collection of administrative information, improving data collection practices and subsequently advancing the existing evidence base concerning family violence in Victoria.
The framework contains information and standards regarding the collection of general and demographic data items, with a particular focus on the community groups identified as a priority by the RCFV and through consultations conducted during the development of the framework. These groups include the priority groups listed in recommendation 204, as well as children and young people who were revealed as a key data gap during consultation.
The purpose of the framework is not to set a standard definition of family violence for government departments, agencies and service providers to use, as this is established through the Family Violence Protection Act 2008 (Vic). Instead, the framework is comprised of a set of data collection standards which organisations can elect to use in order to improve their collection of data concerning family violence. However, the framework is not intended to function as a data dictionary. As such, it is the responsibility of government departments, agencies and service providers to determine how each data collection standard can fit into their data collection guidelines and infrastructure.
The Victorian Family Violence Data Collection Framework focuses on driving improvement in data related to clients and their experiences of family violence. Improvements in the consistency and quality of this information will assist government, agencies and service providers to better understand:
- Who experiences family violence?
- Number of unique people affected (as victim survivors and perpetrators)
- Demographic profile of people involved
- Visibility of priority communities in data
- Barriers to access and need for assistance
- Geographic proximity to client base
- How do people experience family violence?
- Types of family violence experienced
- Persons involved and their role in the family violence
- Characteristics of an event
It should be noted that the framework does not include data items on types of service delivery, outputs or outcomes. Service delivery data items are determined by departments as part of their agreements with service providers. Outcomes specific to family violence are detailed in the Family Violence Outcomes Framework, published in Ending Family Violence: Victoria’s plan for change.
Who is the framework for?
The data collection standards presented in the framework are intended for use by all government departments, agencies or service providers who have the capacity to collect information in the context of family violence.
Figure 1 provides a broad overview of the services that have responsibility for responding to victim survivors or perpetrators of family violence and indicates the types of services the data collection framework is relevant to. This figure uses the four-tier classification originally developed by the Domestic Violence Resource Centre. The RCFV noted that these tiers provide a good starting point for thinking about workforce competencies, and they have been utilised within Building from Strength: 10-year industry plan for family violence prevention and response (Building from Strength) and the Responding to Family Violence Capability Framework.
Tier 1: Specialist family violence and sexual assault practitioners
These specialists spend 90% or more of their time working with victim survivors or perpetrators or engaged in primary prevention activities. Tier 1 practitioners or teams may form part of larger organisations that provide a range of services, or they may be employed in stand-alone services. What they have in common as practitioners is that their sole or major focus is on family violence and/or sexual assault, or on primary prevention.
- Statewide family violence crisis and specialist services
- The Orange Door
- Family violence outreach services
- Women’s refuges
- Centres Against Sexual Assault
- Perpetrator intervention services
- Men’s family violence telephone/online services
- Crisis family violence and sexual assault telephone/online services
- Specialist family violence or sexual assault professionals operating in Tier 2 or 3 services
- Specialist family violence or sexual assault services for Aboriginal or culturally and linguistically diverse women and children or women and children with a disability
Tier 2: Workers in core support services or intervention agencies
Responding to family violence is not the primary focus of these workforces, but they spend a significant proportion of their time responding to victim survivors or perpetrators.
- Courts and court services
- Legal and paralegal agencies and services
- Corrections
- Police
- Family dispute resolution services
- Forensic physicians and medical staff providing sexual assault crisis care
- Child Protection
- Child and Family Services
- Family and relationship services
- Homelessness services
Tier 3: Workers in mainstream services and non-family violence specific agencies
While their work is not family violence, they work in sectors that respond to the impacts of family violence, or in an area where early signs of people experiencing family violence can be noted.
- Health care services
- Drug and alcohol services
- Housing services
- Mental health services
- Centrelink
- Individuals providing therapeutic services
- Emergency services
- Maternal and Child Health Services
- Youth services
- Disability services
- Culturally and linguistically diverse services
- Aboriginal services
- Lesbian, gay, bisexual, trans and gender diverse and intersex services
- Aged care services
Tier 4: Workers in universal services and organisations
Because they interact with children and families in their day-to-day roles, these workers are likely to have regular and extended contact with victim survivors or perpetrators.
Includes workplaces, education services, early childhood services, sport and recreation organisations and faith based institutions.
Figure 1: Workforces that have responsibility for responding to victim survivors or perpetrators. Modified from Building from Strength and the Responding to Family Violence Capability Framework.2, 3
In addition, although the data collection framework was created specifically to improve the quality of family violence data, it may also provide guidance for government departments, agencies and service providers striving to improve the quality and consistency of demographic information, both generally and from priority communities.
Why use the framework?
As previously noted, the RCFV found that there are serious gaps in our knowledge about the characteristics of victim survivors and perpetrators, and about how systems that respond to family violence are working. This is particularly with respect to people from priority communities.
In their report ‘Bridging the data gaps for family, domestic and sexual violence, 2013’, the ABS identified priority themes to improve the evidence base concerning family, domestic and sexual violence in Australia. The priorities identified were to:4
- improve the quality and comparability of existing data sources
- maximise the utility of existing sources
- augment existing data sources to address priority gap areas
The ABS noted the potential of administrative data sources to fulfil the aforementioned data needs. Administrative data are a useful source of information as they utilise existing infrastructure and have the potential to yield information about specific target populations. Data collected in this context are ideal for informing practical decisions about service provision, resource capacity and utilisation, as well as the impacts and outcomes of contact with services.
The content included in this framework aims to meet the priorities identified by the ABS concerning the collection of administrative data related to family violence in Victoria. Standardising the collection of demographic data items and improving administrative data on types of family violence can support broader work to build the evidence base about the impact of family violence on communities.
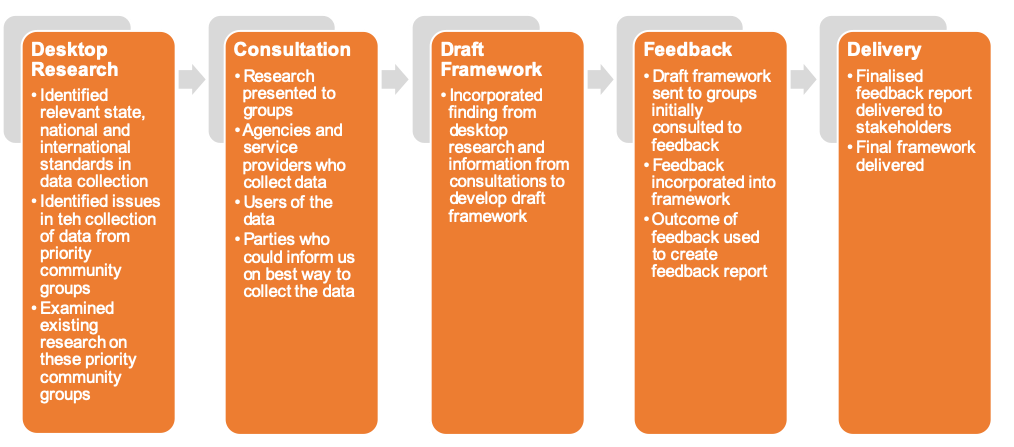
Development of the framework
Figure 2 below shoes the process carried out by the CSA to create the framework. Consultation was an essential part of the development of this framework. For a full list of stakeholders consulted, please see page 109.
2 Department of Health and Human Services (DHHS) 2007, Family Violence Risk Assessment and Risk Management Framework, Victoria, p.9.
3 Australian Institute of Health and Welfare (AIHW) 2018, Family, domestic and sexual violence in Australia 2018, Cat. no. FDV 2, Canberra.
4 Australian Bureau of Statistics (ABS) 2013, 4529.0.00.002 Bridging the data gaps for family, domestic and sexual violence, viewed 12 June 2018, www.abs.gov.au/ausstats/abs@.nsf/Lookup/4529.0.00.002main+features332013
Data collection challenges and improvements
This section identifies common data collection challenges, as well as those more specific to collecting data on family violence, and from priority communities.
Organisations may face a number of challenges in collecting consistent and quality data. To develop methods to improve data collection practices, it is necessary to first identify barriers to consistent data collection. This section identifies common data collection challenges, as well as those more specific to collecting data on family violence, and from priority communities. The section also provides advice about how to address some of these challenges and improve data collection. Government departments, agencies and service providers with responsibility for data collections should consider these challenges and improvement opportunities as part of implementation planning. Additional data collection challenges that are specific to particular communities are discussed in the priority community sections of this paper.
Challenges in current data collection practices
Inconsistent data collection standards
Data standards outline how common data items and demographic information should be collected. Established standards typically contain data definitions, standardised questions and accepted response options which guide consistent collection practices. Currently, there are many national and state-wide data standards which are used for collecting administrative data. These standards are not always broadly applied, and may themselves be inconsistent, and this can impact the comparability of data collections.
For example, many specialist and non-disability specific support services collect data on disability drawing on definitions used by the National Disability Insurance Scheme (NDIS), the National Disability Agreement and state governing bodies. Different types of services may apply different standards depending on what is most relevant for their service provision. For example, medical services may be more likely to collect disability information by way of diagnoses and medical history, while non-disability specific services may be more interested in collecting information concerning support needs or a need for reasonable adjustments. As a result, the scope and detail of information collection may not be consistent across services, making it complex to compare data between services, or to population level data sets.
The absence to date of a co-ordinated effort between government, service providers and other agencies to standardise data collection practices means there is considerable variation in how information is collected and recorded in Victoria in relation to family violence and to priority communities.
Context of data collection
Data collection from clients may occur in a variety of situations and settings where it can be difficult to obtain complete and accurate information, and the amount of information gathered may vary depending on the context of the situation. In most cases, the person responsible for collecting data has a primary role that focusses on the provision of a service (for example, as a police officer, support worker or medical practitioner) and, although they collect data as part of these roles, data collection is not necessarily the primary function of their role. Contexts where certain data collection may be limited include crisis or emergency situations, where workers are prioritising the safety of an individual, or situations where an individual’s privacy may be compromised by asking about family violence, such as in a busy waiting room.
Further, in some cases, organisations may not be resourced to provide services to specific cohorts, which can mean there is little incentive to improve the data collected on these individuals in an administrative setting. For example, some family violence services are not specifically resourced to meet children’s needs and may therefore not collect detailed information on this cohort. Conversely, improved data collection on priority communities can help build an evidence base from which to consider different funding models.
Data collection is not core to business function
The core functions of an organisation and time pressures in service delivery can impact the type and quality of data that an organisation collects. Administrative data are typically collected as a by-product of operational requirements or to meet an internal business need and may only include core information needed to perform a service, such as a client’s contact details. In such cases, information on an individual’s sexual orientation, cultural background or disability may not be seen as an operational requirement for organisations that do not offer specialised services. As a result, organisations may only collect a narrow range of data items, which lack sufficient detail needed for broader secondary use purposes, such as conducting state-wide service analysis, monitoring or research.
A perception that the collection of certain demographic information is not relevant to core business functions can impact data quality and comparability for all priority communities discussed in this framework. For example, while many services are legally obliged to collect information on a person’s requirement for an interpreter, other information on their cultural background may not be deemed as relevant to service delivery, resulting in partial information on CALD communities. Concerns have also been raised about how the collection of Aboriginal information may contravene an organisation’s commitment to equitable service delivery5, despite the fact that a person’s response to this question should not impact the standard of service they receive.
Complexity
In some cases, adequate information about a person’s background cannot be ascertained through one data item, for example for CALD and LGBTI communities, and for people with disabilities. Where this is attempted, it often under-represents those who face heightened risks and barriers to accessing services. It also has the potential to add confusion regarding different concepts that may not be fully understood by people outside of specific communities. For example, grouping diverse people and communities into a single ‘LGBTI’ group, or using the need for an interpreter as a marker of CALD communities, does not recognise and represent these communities accurately, and decreases data integrity.
Lack of training in data collection
As the primary role of front-line service and clinical staff will generally not be data collection, they may not receive training in this area. If staff do not receive training or understand why they need to collect particular data, they may feel less confident to ask the associated questions, or ask them in a different way. A lack of training in how and why to collect certain kinds of data can particularly impact the priority communities discussed in this framework. For example, given the personal nature surrounding questions about sexual orientation or intersex variation, organisations may be reluctant to ask for this information, particularly if there are concerns that this may cause a person to be offended or experience discomfort. A fear of causing offence may also impact staff willingness to ask questions about a person’s disability, cultural background or Indigenous status, and lead them to make assumptions based on observation or on information being volunteered. Staff training in the benefit of collecting these data items, and in sensitive or culturally appropriate ways to do so, can build staff understanding of the value of these types of data, and assist in building data quality and consistency.
Lack of quality assurance processes
There may be limited opportunities to confirm information with a person who has been in contact with a service, meaning that the data initially collected cannot be verified. Additionally, the sophistication of record keeping systems can vary and data quality is often reliant on the person entering the data correctly. Depending on the resourcing of an organisation, time may not permit staff to review information for completeness and obtain missing data.
Changes to definitions and policies and maintaining data comparability
Over time, best practice data collection policies and procedures change. Agencies and their staff may not be aware of these changes and how they affect them, meaning that they inadvertently follow outdated practices. This issue tends to be more prevalent in large organisations, particularly if information is not communicated widely and consistently throughout the workplace. Also, if training is not provided to reinforce changes in practice, staff may continue to follow the procedures they are most familiar with.
Organisations changing data collection systems and processes also need to be aware of the need to ensure continuity of reporting using existing data items. For example, many service providers are bound by the requirements of their funding body to provide particular data fields on a regular basis. Furthermore, in some cases these minimum requirements are established at the federal level, rather than by Victorian state government departments. Longitudinal analysis of service usage based on common data items, and comparability to national data sets, such as those of the ABS, are another consideration when updating data collections.
Economic and IT restrictions
Some organisations may not have the capacity or infrastructure to prioritise improvements to data collection systems and processes. This may be due to a backlog of paper-based records to be digitised, a small workforce to input and maintain data, and lack of budget to upgrade records management systems. It is also important to note that many IT systems are provided by government departments, who also carry the responsibility of resourcing and conducting system updates. These updates can be expensive and take time. In some cases, these IT systems may have limited capacity to include multiple response values or dynamic questioning, that supports sophisticated data collection. The introduction of multiple response options may also present problems for exporting and analysing data.
Improving data collection
The remainder of this section provides information on improving data collection practices in general. It includes a range of processes that can be implemented at the organisational level, and through changes in infrastructure and data collection practices. It also provides advice on interim process for improving data quality for analysis and reporting purposes, and information on privacy and security requirements.
Organisational Practices
Commitment from all levels of an organisation to improve data collection
Improving data collection and the quality of data holdings requires a concerted effort from an entire organisation, and should begin with a top-down commitment for change. This includes identifying priority areas for improvement and barriers to improvement, adopting best practice procedures for collecting quality data, using data standards where available (including those recommended in this framework), ensuring IT infrastructure is kept up to date and allows for efficient and effective data collection, and providing training where needed to those collecting data to ensure confidence and consistency in data collection practices.
Training
It is important to provide training to staff involved in the collection of data. Training should emphasise why it is important to collect data and highlight the benefits of data for operations, planning, research and evaluation. If staff understand the rationale for collecting certain information, they will feel more confident to ask for these data items and to explain why it is important. Training should include how to phrase questions, clarify answers and record responses.
Using data-related Key Performance Indicators (KPIs)
Setting KPIs linked to data and evidence can be a motivating factor for organisations to ensure improvement in their data collection practices. KPIs can target many aspects of data quality including completeness (how many records have a recorded value), and precision (how many records have a meaningful or valid value). Organisations should set reasonable KPIs that aim to improve the quality of their data, but not create perverse incentives that could undermine data quality or service delivery.
For example, an organisation finds that only 50% of the clients contained within their record management system have a recorded gender. The organisation sets a KPI for 100% of clients to have a recorded gender, and they monitor this goal over the course of a six-month period to ensure that improvements made are effectively moving towards this goal.
Conducting audits and business process reviews
If possible, it is recommended that audits of datasets are conducted at regular intervals to ensure accuracy and completeness of recorded data. Audits may illuminate systemic or recurring issues in data collection that can be addressed once identified. Similarly, reviews of business processes can identify difficulties in data collection and assist an organisation to understand the barriers to quality data collection. Conducting audits and business review processes can also be a component of evaluating the success of KPIs.
Infrastructure and Collection Practices
Data items have pre-defined responses
Where appropriate, it is recommended that data items have a pre-defined set of response options at the point of entry into a data management system. This reduces the potential for typographical errors and enables more efficient data collection and subsequent analysis. However, there may be instances where a free text field should be provided. Recommended response options and instances where free text coding should be allowed will be discussed in the data collection standards proposed in this framework.
Accommodation of multiple response options
There are some priority data items where it is not ideal to collect only one response from a person. For example, when asking a person to describe their disability, a person may disclose that they are blind and have mobility difficulties. In this case, it may be restrictive to ask someone to choose between response options when recording their disability type. It is acknowledged that allowing for multiple response options can create complexities both for IT infrastructure and for analysis of the collected data, however it is recommended that for certain data items, agencies and services consider approaches which accommodate multiple response options.
Creating mandatory data fields
Where appropriate, it is advised that service providers and agencies update their data collection infrastructure to utilise mandatory data fields (or at minimum, prompts, on all non-optional data items). Therefore, the person inputting the data cannot move to the next screen without entering a response in mandatory data fields. Incorporating mandatory data fields into a records management system ensures that all non-optional data items receive a response. However, it is important to remember that people have the right to not respond to a question.
For example, to improve their collection of gender information, an organisation updates their data entry system so that a response for gender must be recorded when entering details about a new client before the new entry can be completed. The organisation now finds that 100% of all new client records have a recorded response for gender.
Guidance for collecting data in written form and verbally
Regardless of whether data collection is written (form-based) or verbal, using the question phrasing and response options outlined in each data item is recommended. Further, it is generally recommended that data are collected directly from a client, rather than by proxy, particularly for sensitive information such as a person’s sexual identity or orientation.
| Collecting data via a third party |
|---|
| Although it is preferable for data to be gathered directly from a person, this may not always be possible. Agencies and services should have their own policies which dictate where it is acceptable for communication (and by proxy, data collection) to take place through an agreed upon third party. Agencies and services should be aware that in some cases a person’s guardian or representative may be the perpetrator of family violence against that person. If such a circumstance is suspected, agencies and services are encouraged to have protocol in place to help assist victims so that the offending party is not speaking on behalf of the victim. |
Where data are collected from a respondent verbally, questions should be asked as they are written, and data collectors should describe the response options available for each question. Detailing the full list of response options across data items can have a range of benefits, including communicating that an organisation is inclusive of a broad range of identities, as well as assisting respondents with choosing the most appropriate category for them. In some cases, such as for the disability data items, respondents may need additional information to understand the scope of categories, and data collector should provide information and guidance to assist with understanding each of the categories.
Where possible, all available categories in a data item or classification being used should be read or provided to a respondent rather than a short-list. However in cases where the context of the data collection does not allow for this, the question can be asked on its own. Managing long lists of response options is particularly relevant to questions about country of birth and language spoken at home, where there is an extensive range of options a person may choose. If a short-list is being used, and a respondent’s answer is a category in the short-list, this category should be selected. Where their answer is not in the short-list of response categories, the data collector can select ‘other’ and where possible, enter the response in the text field.
Because communities may have unique, or an extensive range of terms to describe identities, such as sexual identity or ethnicity, it may be necessary to clarify the term used with the respondent. For example, if a client responds to a question on gender identity as ‘non-binary’, the data collector should confirm with the client that this aligns with the ‘self-described’ response category, and write ‘nonbinary’ in the free text field which accompanies that option. Responses should not be questioned or assumed based on a person’s appearance or other information that has already been disclosed.
Including response options for ‘prefer not to say’, ‘question unable to be asked’ and ‘no response’
Inevitably, there are circumstances where it is not possible to obtain certain information. It is recommended to include response options for priority items that will help provide details about why information was not able to be collected. This can be used to evaluate collection practices, and determine if solutions can be implemented to better address gaps in data. There are some data items that may involve the disclosure of sensitive information. Hence, it is recommended to provide respondents with a ‘prefer not to say’ option, which respects a person’s choice not to disclose particular information. Including this as an option also enables data analysis to determine where the question was asked and the response is not missing or unknown for other reasons.
When questions are asked of people verbally, it is possible that the data collector will be unable to gain all the required information. This may be due to the context in which the information is being gathered (for example, an emergency event), or to other unexpected events (for example, a client abruptly hangs up the phone). In these cases, it is ideal to include the response option ‘question unable to be asked’, which explains why the information was unable to be recorded.
When questions are asked of people by form or online, a person may choose to not complete all questions. In these cases, it is recommended to include a response option for ‘no response’, for when this information is subsequently lodged in a data records system.
For example, an organisation is pleased to find that they have achieved their goal of 100% of all clients having a recorded gender. Upon closer analysis of the records however, the organisation finds that 40% of the records have a gender recorded as ‘unknown’. As all data are collected verbally from clients, they update their records management system to allow for response options for ‘prefer not to say’ and ‘question unable to be asked’. Over time, they find that for 30% of all clients, a question about their gender is unable to be asked.
Following up to obtain additional data
It is acknowledged that certain situations do not permit the collection of comprehensive data. Where feasible, it is recommended that missing data are followed up at an appropriate time. In particular, organisations that work with people in a crisis or emergency situation should obtain data required to deliver the immediate service, and then follow up for further information once the crisis or emergency has been managed. The follow up to address data gaps could accompany an existing operational task, including a routine call to ensure the welfare of a patient or client following a service.
For example, an organisation finds that 30% of their client records have a response value of ‘question unable to be asked’ for gender. After consulting with front-line staff, it emerges that information is typically gained from clients while they are accessing an emergency service. The organisation may decide it is appropriate to implement a follow up later which includes collecting missing data items.
Interim improvements for analysis and reporting purposes
Improving the quality of demographic data within one data source
In cases where clients are presenting over multiple occasions and there is partial coverage of a data item, there are post-hoc data improvement processes that can be implemented to superficially improve the quality of the data. It is important to note that historical responses to data items should remain unchanged, and the application of any of the methods below should update only the most current status. There are three options to improving the quality of demographic data, all of which have advantages and disadvantages. These rules that summarised below are drawn from the CSA’s ‘Consultation paper: Improving recorded crime statistics for Victoria’s Aboriginal community’6. However, the approach is more broadly relevant to other demographic identifiers:
- Application of an ‘ever-identified’ rule - Using this method, a person who has identified at one point in time as being of Aboriginal would then be given this status across all of their other records in the database.
- Application of a ‘most recent identification’ rule - Using this method, a person’s most recent Indigenous status would be applied across all of their other records in the database.
- Application of a ‘most frequent’ rule - Under this method, a person’s most frequent response to the SIQ would be applied across all of their other records in the database.
For the purposes of analysis and reporting on Victoria Police crime data, the CSA applied the ‘most frequent’ rule to Indigenous status to improve the quality of the Indigenous status variable in victim and offender analyses. Overall, feedback received by the CSA indicated that this rule was the favoured methodology.7 This concept can be applied across other datasets where individual clients can be identified across a database and would provide an interim measure while other data improvement processes are developed and implemented.
Improving the quality of data across multiple data sources
In addition to using one of the methods outlined above, it is also possible to use multiple data sources to identify a person’s certain demographic or community data items even where it is not directly collected as a result of a service or business process. This involves linking a person across the datasets using key pieces of information and attributing that data category in one data source to their profile in another source.
Privacy and security considerations
This section outlines some of the privacy principles that public sector organisations should be aware of when collecting and storing data. If policies and procedures regarding the secure storage and transfer of data are not already in place, organisations may be reluctant to collect personal information if it is not imperative for their operations. However, this section is not intended to provide extensive privacy and security guidance; instead organisations should refer to any relevant legislative, regulatory and administrative provisions for further information.
Information Privacy Principles (IPPs) and Health Privacy Principles (HPPs) are privacy principles which govern the way that public sector organisations, including contracted service providers, collect, use and handle personal and health information. The IPPs apply to personal information under the Privacy and Data Protection Act 2014 (Vic) (PDPA), while the HPPs apply to health information under the Health Records Act 2001 (Vic) (HRA).8 Privacy principles that are particularly relevant to the framework include; IPP/HPP 1 (Collection), IPP/HPP 3 (Data quality), IPP/HPP 4 (Data security), IPP/HPP 8 (Anonymity), and IPP 10 (Sensitive information).
The Office of the Victorian Information Commissioner has developed the Victorian Protective Data Security Framework (VPDSF), which provides comprehensive information on managing data security risks from the point of data collection and throughout the information lifecycle.9 The standards in the VPDSF relate to data governance, information security, personnel security, Information Communications Technology security, and physical security. It is recommended that organisations review and adopt these protocols prior to data collection.
In addition to the IPPs and HPPs, there are a number of other policies and laws that make up the Victorian information management landscape, which agencies should consider when developing their own privacy and security policies. In particular, organisations should turn to their enabling legislation as a starting point in determining the information they are permitted to collect.
In particular government departments, agencies and service providers should be aware of their obligations where prescribed under the Family Violence Information Sharing Scheme (FVIS Scheme) and the Child Information Sharing Scheme (CIS Scheme)10. The FVIS Scheme and CIS Scheme are aimed at removing barriers to information sharing to allow professionals to work together across the service system, to make more informed decisions and better respond to the safety and wellbeing needs of individuals, children and families. The requirements of Schemes, including record keeping requirements, are detailed in the Family Violence Information Sharing Guidelines and the Child Information Sharing Guidelines. When services are sharing information under these schemes, the Victorian Protective Data Security Standards will continue to apply.
Organisations are encouraged to seek advice prior to implementating the data items proposed in this framework to ensure compliance with relevant privacy legislation. Individual organisations are responsible for ensuring that their business practices are compliant with State and Commonwealth privacy requirements and information sharing schemes, and should seek guidance from privacy advisors, legal teams, the Office of the Victorian Information Commissioner and/or the Health Complaints Commissioner when unsure about their obligations.
5 AIHW 2010, National best practice guidelines for collecting Indigenous status in health data sets, Cat. no. IHW 29, Canberra, p.3.
6 CSA 2016, Consultation paper: Improving recorded crime statistics for Victoria’s Aboriginal community, viewed 22 June 2018,
www.crimestatistics.vic.gov.au/about-the-data/consultation-paper-improving-recorded-crime-statistics-for-victorias-aboriginal(opens in a new window)
7 CSA 2016, Outcomes of recent public consultation: proposed methods to improve Victorian Aboriginal and Torres Strait Islander
recorded crime statistics, viewed 22 June 2018, https://www.crimestatistics.vic.gov.au/media-centre/news/outcomes-of-recent-public-consultation-proposed-methods-to-improve-victorian(opens in a new window)
8 Commissioner for Privacy and Data Protection 2016, Information sheet: Information Privacy Principles and Health Privacy Principles – May 2016, viewed 12 June 2018, www.cpdp.vic.gov.au/menu-resources/resources-privacy/resources-privacy-…
9 Office of the Victorian Information Commissioner 2018, Victorian Protective Data Security Framework – March 2018, viewed 20 June 2018, www.cpdp.vic.gov.au/menu-data-security/victorian-protective-data-security-framework/vpdsf(opens in a new window)
10 Department of Education and Training, The Child Information Sharing (CIS) Scheme and The Family Violence Information Sharing (FVIS) Scheme available at https://engage.vic.gov.au/child-information-sharing-scheme(opens in a new window)
Data collection standards - General data items
This section discusses the importance of collecting general data items.
This section discusses the importance of collecting general data items, and presents existing national standards which should be used to ensure consistent and high quality collection of data by Victorian government departments, agencies and service providers.
Individual and demographic data items
Collecting information from people who come into contact with agencies and service providers is often a balancing act between respecting the privacy of individuals, gaining enough information to perform core business functions, making informed decisions about service use, and providing a deeper understanding about the experiences of people affected by family violence. Individual and demographic information is particularly valuable for creating a demographic profile of those affected by family violence, and is therefore essential in improving the family violence evidence base in Victoria. This section highlights data items which can be used to improve the quality and consistency of individual and demographic information on people who come into contact with an agency or service.
Names
Details about a person’s name are commonly collected by agencies and service providers. This information can be used by organisations as the primary identifier of a person’s identity, and is often necessary when seeking to count unique individuals who come into contact with an agency or service. Names are also an important component for data linkage projects, which are increasingly becoming a priority across government departments in Australia, enabling improved understanding of client pathways across agencies and services. It is therefore important that name information is collected consistently and accurately. The Commonwealth Attorney-General’s Department recognised the need to capture accurate and detailed information on people’s names, and published better practice guidelines for the collection of identity data in 2011.11 While these guidelines are targeted at Commonwealth agencies, the document sets out several principles that are valuable for all agencies and services that collect name information for the purpose of establishing identity. Some of the key principles in these guidelines are outlined below.
Information should be collected whenever possible. While there are some contexts where collection of a person’s name may not be appropriate, including where services are provided anonymously, information should be collected about a person’s first and last name whenever a person consents to provide it.
Information should reflect what is written on an official ID document. In order to ensure that information collected on names is done so uniformly and accurately, given names and family names should be recorded as they are written on an official government identification document. Data collectors should avoid recording nicknames, initials or abbreviated names in the given and last name fields, and instead, these should be captured in separate data fields. Whenever possible, nonalphabetical features should be collected as they appear in a name on official identification (including hyphens and spaces), as this is a feature which can improve the uniqueness of collected names.
It is noted that asking people to produce an ID document to verify their name may present a number of operational challenges or may not be possible given the nature of some services (for example, telephone-based services). A requirement to provide an official ID document may be challenging or offend people from some priority communities. For the reasons discussed, it is important to collect name information as recorded on official ID documents. However, unless official identification is required to be sighted by a service, it is recommended that people are not asked to provide an ID document to verify their name.
Additional name information should be collected. People frequently use names other than the name recorded on their identification document. If a person has a nickname or different name they use, this information should be collected in addition to the name appearing on their identification document. Staff should use this name during all communications with that person.
Please note that when asking if someone uses a different name than what is recorded on their identification document, it may be considered offensive to ask what their ‘preferred’ name is. This is particularly true for some trans and gender diverse people, and as such it is not recommended that agencies use the word ‘preferred’ when asking about the name that a person uses. For more information, please see the LGBTI communities section of this framework, which provides specific advice regarding the collection of information from LGBTI people.
Examples of name questions:
What is your given name[s], as it is recorded on government issued ID?
What name do you use? [if different from given name/s]
What is your family name, as it is recorded on government issued ID?
Name usage type. To assist with differentiating between the types of names collected, agencies or service providers may elect to use a data item which indicates the type of name used. Name usage type (METeOR identifier: 453366) concerns the usage type of a person’s family name and/or given name and enables differentiation between each recorded name.12
Records should be updated where appropriate and historical records retained. It is acknowledged that people often change the name that is recorded on their official ID document for a variety of reasons. Name information should be kept up-to-date to reflect the current information recorded on a person’s identification documents. Wherever possible, historical records of a person’s name should be retained, as this provides greater potential to confirm a person’s identity.13
Age / Date of birth
Age is a widely collected data item across agencies and service providers, however the method by which it is collected varies. Some offices collect age as a discreet number (for example, ‘65’), a predefined group (for example, ‘60 and older’) or as a date of birth which is later used to derive a person’s age.
The standard recommended in this framework is to collect age in the form of an individual’s date of birth. Date of birth should be collected in accordance with the format described by METeOR identifier 287007, which is DDMMYYYY. Collecting date of birth has the advantage of providing more detailed and accurate information about a person’s age, and it can be used for other purposes, including identifying unique individuals and linking datasets. The ABS has noted that “collecting age in complete years can lead to an error where a respondent may round off or approximate their age”.14 Additionally, collecting age as a number fixes a client age to the year in which it was collected, and the information loses meaning if it is unclear when the age was recorded. This is particularly true when a client interacts with an organisation over a long period of time.
Wherever possible, an agency should ask for the date of birth that an individual uses on their official ID documents. As with name information, unless official identification is required to be sighted by a service, it is recommended that people are not asked to provide an ID document to verify their date of birth.
It is noted that there are instances where an individual may not know their birth date, or where they are only able to supply a numerical estimate of their age. The date of birth standard used in a number of national minimum datasets (METeOR identifier: 287007) suggests that if date of birth is not known or cannot be obtained, provision should be made to collect or estimate age. Collected or estimated age would usually be in years for people 2 years and older, and to the nearest 3 months (or less) for children aged less than 2 years old. An estimated date of birth may also be relevant for unborn children. A child believed to be aged 18 months in January 2018 would therefore have an estimated birthdate of 01062016.15
When a recorded date of birth has been estimated, it is recommended that an indicator is used to denote that the date is an estimate. Information regarding best practice for indicating estimated dates is discussed later in this section.
Example of age question:
What is your date of birth [as it is recorded on your birth certificate or other form of identification]? DDMMYYYY
Date variables
Most organisations who collect data will record some type of date information. This can include the date when a service was initiated, attended and completed, when family violence was disclosed, when a family violence incident occurred, or, as previously noted, date of birth. To ensure that high quality date information is collected, it is recommended that dates are completed in full whenever possible, and contain an accurate record of the day, month and year.
In Australia, the date format most commonly used is DDMMYYYY. It is recommended that information is collected and stored in this format.
Finally, it is recommended that organisations collect a ‘create date’ or similar data item. This date represents the date an electronic record is created to be stored in an administrative data collection system. It is strongly recommended that the create date is auto-generated at the time that a case or record is first created. If records are promptly entered into a records management system, this approach ensures that the date is consistently and accurately collected.
Estimated dates. When a date is estimated, agencies and service providers are encouraged to use a data item which indicates that the date is an estimate. When estimating dates, Date – accuracy indicator (METeOR identifier: 294429) can be utilised to indicate which parts of the recorded date are known, estimated and unknown. The table below depicts how three codes are used in combination to provide information about the accuracy of a recorded date. For a full list of response options, please see the METeOR website.16
| Data domain | Day | Month | Year |
|---|---|---|---|
| Accurate | A | A | A |
| Estimated | E | E | E |
| Unknown | U | U | U |
Gender identity and sex
Most agencies and service providers will collect information on a person’s sex or gender identity. Due to the overlap between these data items and information concerning LGBTI communities, the standard suggested for collecting this information is described in detail in the LGBTI communities section of this framework.
Geographic variables
Agencies and service providers may collect a range of geographic information surrounding family violence, depending on their operational purpose and the services that they provide. Examples of geographic data collected include the home address of a victim-survivor or perpetrator (person address) and the address of where a service is provided (organisation address).
Many agencies and service providers will collect geographic information as aggregated regions, for example, Local Government Areas (LGAs) or Department of Health and Human Services (DHHS) service regions. While this information may satisfy internal demands, it can have limited value for research purposes or when looking to compare data with population-based statistics. Additionally, geographic areas such as LGAs and other administrative service regions change over time.
Collecting detailed geographic information allows data to be mapped to higher level geographic structures as needed, such as those that exist in the ABS Australian Statistical Geography Standard (ASGS) 2016.17 The ‘Address Details Data Dictionary’ (METeOR identifier: 434713) created by the AIHW sets out address information which is important to collect for these purposes. As recommended by the data dictionary, when collecting information on addresses agencies and service providers should collect primary address information. This includes:18
- address site (or primary complex) name
- address number or number range
- road name (name/type/suffix)
- locality
- state/territory
- postcode
- country (if other than Australia)
In 2010, DHHS released their ‘Address reference data dictionary (version 1.1)’,19 which provides a common set of concepts, data elements and edit/validation rules that define the basis of address data collection. If interested in collecting data elements outside of the primary address information listed above, this data dictionary draws on existing national standards to assist data collection custodians to better document and manage address data. It is therefore a valuable resource for agencies and service providers to consider when seeking to align their address data items with national standards.
Unique identifiers and data linkage considerations
Unique identifiers
Unique identifiers (UIDs) can be used in a variety of contexts, but typically their purpose is to identify a unique item, person or case file. Often UIDs will consist of a distinct combination of letters and numbers that are randomly assigned and auto-generated by a records management system, however they may also be borrowed from other forms of identification codes. For example, some services may use a person’s driver’s license or passport number as their UID, or they may adopt a UID given by a different system (for example, courts may use the person identification number created by Victoria Police’s Law Enforcement Assistance Program (LEAP) system).
Examples of unique identifiers:
Case file number: C14-12-002 Client number: Z103903
Where UIDs are used, it is recommended that agencies and service providers ensure that the numbers given to clients are always unique, and that there is a protocol in place to prevent UIDs or clients from being duplicated.
The Office of the Victorian Information Commissioner has created an Information Sheet concerning the use of UIDs and relevant considerations under the Privacy and Data Protection Act 2014 (Vic).20 Organisations should review their obligations under relevant legislation in Victoria when considering implementing the use of UIDs for identifying individuals.
Statistical Linkage Key (SLK): As described by the AIHW in METeOR identifier 686241, an SLK is a key that enables two or more records belonging to the same individual to be brought together. It is a 14 character string represented by a code consisting of the second, third and fifth alphanumeric characters of a person’s family name, the second and third alphanumeric characters of a person’s given name, the day, month and year when the person was born (in the format DDMMYYYY) and a single alphanumeric character representing the sex of a person, concatenated in that order:21
XXXXXDDMMYYYYX
SLKs are valuable for collection because they not only serve as unique identifiers which assist with counting unique people accessing a service, but as they are uniformly created, they can be used to link individuals across internal and external data sets.
Data linkage
The potential to link datasets between agencies and service providers is becoming a matter of priority in Australia. Recommendation 204 of the RCFV specifically mentions the need to explore “opportunities for data linkage between existing data sets...to increase the relevance and accessibility of existing data”.22 Data linkage can also provide greater insight into perpetrator and victim-survivor engagement with services, and an opportunity to view an individual’s trajectory through the criminal justice and community services systems.
The most significant data items which assist with data linkage are those that can be used to denote unique individuals, cases, times and locations. Often the most desirable information which can be used for this purpose are high quality UIDs. Specific details concerning UIDs are described earlier in this section, however it is worth noting that for linkage purposes, the collection of external UIDs in combination with internally created UIDs is ideal. For example, a service may receive an L17 Risk Assessment and Management form from Victoria Police as part of an application or a referral for service, and where possible, agencies should collect the incident number that is recorded on this form, in addition to creating their own file ID and client ID. Retaining the incident number assigned by Victoria Police will allow for data collected by a service to be easily and reliably linked back to Victoria Police data if required.
Other data items can be used for linkage purposes if they are collected in a consistent and accurate manner. These items include first and last name, date of birth and sex or gender information. Best practice methods for collecting this information are described earlier in this section.
11 Department of Home Affairs 2011, Improving the Integrity of Identity Data: Recording of a Name to Establish Identity 2011,
Attorney-General’s Department, viewed 12 June 2018, www.homeaffairs.gov.au/about/crime/identity-security/guidelines-andstandards
12 AIHW Metadata Online Registry, Person – name usage type, code AAA, viewed 20 June 2018,
http://meteor.aihw.gov.au/content/index.phtml/itemId/453366
13 Department of Home Affairs 2011, Improving the Integrity of Identity Data: Recording of a Name to Establish Identity 2011,
Attorney-General’s Department, viewed 12 June 2018, www.homeaffairs.gov.au/about/crime/identity-security/guidelines-andstandards
14 ABS 2014, 1200.0.55.006 Age Standard Version 1.7, viewed 20 June 2018, www.abs.gov.au/ausstats/abs@.nsf/Lookup/1200.0.55.006main+features72014,%20Version%201.7
15 AIHW Metadata Online Registry, Person – date of birth, DDMMYYYY, viewed 12 June 2018,
http://meteor.aihw.gov.au/content/index.phtml/itemld/287007
16 AIHW Metadata Online Registry, Date – accuracy indicator, code AAA, viewed 12 June 2018,
http://meteor.aihw.gov.au/content/index.phtml/itemld/294429
17 ABS 2016, 1270.0.55.001 Australian Statistical Geography Standard (ASGS): Volume 1 – Main Structure and Greater Capital City Statistical Areas, viewed 20 June 2018, www.abs.gov.au/ausstats/abs@.nsf/mf/1270.0.55.001
18 AIHW Metadata Online Registry, Address details data dictionary, viewed 20 June 2018,
http://meteor.aihw.gov.au/content/index.phtml/itemId/434713
19 DHHS 2010, Address reference data dictionary version 1.1, viewed 20 June 2018, www2.health.vic.gov.au/about/publications/policiesandguidelines/data-dictionary-address-reference
20 Commissioner for Privacy and Data Protection 2017, Information sheet: ‘Unique Identifier’ under the Privacy and Data Protection Act 2014 (Vic), viewed 12 June 2018, www.cpdp.vic.gov.au/menu-resources/resources-privacy/resources-privacy-information-sheets
21 AIHW Metadata Online Registry, Record – linkage key, code 581 XXXXXDDMMYYYYX, viewed 13 June 2018,
http://meteor.aihw.gov.au/content/index.phtml/itemld/686241
22 RCFV 2016, Summary and recommendations, Victoria, p.101.
Data collection standards - Family violence data items
Introduces a set of family violence data items that are intended to support consistent recording of core information concerning family violence.
The RCFV identified a range of gaps in family violence data and in systems for comprehensively recording and assessing data. Some of these gaps stem from under-recording and hidden reporting of family violence, and others from limited demographic information and inconsistent definitions in collecting data. This section introduces a set of family violence data items that are intended to support consistent recording of core information concerning family violence. This includes the type of family violence, the relationships between the person using family violence and those affected by it (namely, nature of the familial relationship), and whether the person accessing the service at a particular point in time is identified as the victim or perpetrator of family violence.
The questions and responses included in this section are not intended to function as a check-list to determine whether or not an incident constitutes family violence. Nor are they intended to assist staff in identifying if a client is at risk of family violence. Their purpose is to operate as a defined set of data items that will support greater consistency in recording information about family violence in administrative data.
A range of work is underway as part of the Victorian Government family violence reforms to support organisations and practitioners to better understand, identify and respond to family violence. This includes workforce training and development activities detailed within Building from Strength and within the Responding to Family Violence Capability Framework. The Family Violence Multi-Agency Risk Assessment and Management Framework (MARAM) provides tools and guidance for organisations and professionals on how to identify and assess family violence and risk; and how to respond within their legal obligations. MARAM provides evidence-based family violence risk factors, and questions to support identification and assessment of family violence risk, and is a useful references for departments, agencies and service providers on best practice standards for identifying and responding to family violence risk.
| Family Violence Risk Assessment and Risk Management Framework |
|---|
|
The Family Violence Multi-Agency Risk Assessment and Management Framework has been established in law under a new Part 11 of the Family Violence Protection Act 2008 (Vic). This requires organisations that are prescribed through regulations, as well as organisations providing funded services relevant to family violence risk assessment and management, to align their policies, procedures, practice guidance and tools to the MARAM Framework. The MARAM Framework provides policy guidance to organisations prescribed under regulations that have responsibilities in assessing and managing family violence risk. It provides support to organisations and professionals to recognise a wider range of presentations of risk for children, older people and diverse communities, across identities, family and relationship types and will keep perpetrators in view and hold them accountable for their actions and behaviours. Under MARAM:
|
Terminology and definitions
Defining family violence
Family violence is behaviour that controls or dominates a family member and causes them to fear for their own or another person’s safety or wellbeing and includes exposing a child to these behaviours. Family violence presents across a spectrum of risk severity, from subtle exploitation of power imbalances, through to escalating patterns of abuse over time.
The Victorian Family Violence Protection Act 2008 (Vic) (FVPA) uses broad definitions of family violence and ‘family’ or ‘family-like’ relationships.
| Definition of family violence |
|---|
|
The FVPA identifies family violence as – (1)(a) behaviour by a person towards a family member of that person if that behaviour – (i) is physically or sexually abusive (b) behaviour by a person that causes a child to hear or witness, or otherwise be exposed to the effects of behaviour referred to in paragraph (a).23 Examples of family violence that are referred to in the FVPA include:
|
Family violence is much broader than the physical component that is commonly associated with the term. It is vital that organisations working with clients affected by family violence understand all the types of violence experienced by their clients. This is particularly important for abuse which is harder to recognise, including controlling behaviours, isolation, sexual assault, financial, emotional and spiritual abuse. Acts of family violence may constitute a range of criminal or civil offences. The MARAM Framework outlines all family violence risk factors, which individually or in combination are used to identify the presence of family violence risk. MARAM risk factors are the basis upon which family violence risk is assessed in Victoria. The MARAM risk factors can be categorised into the forms of violence in the Family Violence Protection Act 2008 (Vic) (outlined above) and which relate broadly to the data items listed below. There are other forms of family violence which are not included in the brief examples below, such as stalking (including through use of technology or social media) and theft.
Physical abuse
Physical abuse refers to abuse involving the use of physical force against another person. Physically abusive behaviours can include shoving, hitting, slapping, shaking, throwing, punching, biting, burning, strangling or poisoning, including use of weapons or objects to cause physical harm.24 It can also include lack of consideration for a victim’s physical comfort or safety (such as dangerous driving). Some acts are physically abusive even if they do not result in physical injury.
Sexual abuse
Sexual abuse refers to forcing a person to engage in sexual activity.25 Sexual abuse can include rape, forcing a person to perform sexual acts, causing a person pain during sex without their consent, and forcing a person to watch pornography. Being pressured to agree to sex, unwanted touching of sexual or private parts, causing injury to the victim’s sexual organs are all examples of sexual abuse. Sexual abuse includes sexualised behaviours towards an adult or child, such as talking in a sexually explicit way, sending sexual messages or emails, exposing to sexual acts, having a person pose or perform in a sexual manner when they do not want to, or are unable to consent to do so.
Emotional / psychological abuse
The FVPA defines emotional or psychological abuse as a behaviour that torments, intimidates, harasses or is offensive to another person. Emotional abuse refers to ‘abuse that occurs when a person is subjected to behaviours or action (often repeatedly) aimed at preventing or controlling their behaviour, with the intent to cause them emotional harm or harm through manipulation, isolation or intimidation.26 Any form of behavior that deliberately undermines the victims confidence, acts to humiliate, degrade or demean the victim. This includes threats to the person or their friends or family, or for a perpetrator to threaten to commit suicide or self harm. Silence and withdrawal are also means of abuse.
Emotional abuse may be verbal or non-verbal. Forms of emotional abuse include, but are not limited to, verbal abuse or insults, including racial, homophobic and transphobic taunts, restricting a person’s freedom, threatening deportation or to withdraw support for immigration applications, threatening to report a person to Centrelink or other authority, threatening to disclose a person’s sexual orientation against their wishes, isolating someone from their family and friends or preventing a person from expressing their cultural or spiritual identity, threatening suicide, threatening harm to family members or pets, threatening the loss of custody or access to children, or blaming someone for problems and making them feel guilty. Social, spiritual and cultural abuse are specific kinds of emotional or psychological abuse, and are described in more detail below.
Social abuse
Social abuse is a form of emotional/psychological abuse, however it specifically focuses on creating a sense of social isolation for the victim-survivor. Social abuse is preventing a person from having contact with relatives, friends, service providers and other people, or restricting a person’s activities to increase their sense of social isolation.27 Social abuse can include confining a person to their home or room, preventing a person from answering the phone or door, stalking, intentional embarrassment in front of others, including revenge porn, posting private or sensitive information about a person online without their permission, or threatening to reveal personal details about a person such as their sexual orientation to others. Continually putting friends and family down so the victim is slowly disconnected from their support network, or preventing contact with people who are in a person’s cultural, linguistic, faith or other identity community are forms of social abuse.
Spiritual / cultural abuse
Spiritual or cultural abuse occurs when power and control is used to deny a person their cultural or spiritual rights and needs.28 Like social abuse, spiritual and cultural abuse is as a form of emotional or psychological abuse. It can include using religion or culture as an excuse to commit particular abuse or to justify the behaviour. Other examples of cultural or spiritual abuse include denying access to cultural or spiritual ceremonies or rights, preventing religious observances or practices, forcing religious ways and practices against a person’s own beliefs, and denying a person their cultural heritage. Spiritual and cultural abuse overlap with the concepts of and emotional/psychological abuse, however they are unique by their use of spirituality or culture as a component of the abusive behaviour. Ridiculing or putting down a victim’s beliefs or culture. Preventing them from belonging to or taking part in a group that is important to their spiritual or cultural beliefs, or practicing any faith or religion.
Economic / financial abuse
The FVPA defines economic abuse as, behaviour by a person (the first person) that is coercive, deceptive or unreasonably controls another person (the second person), without the second person’s consent –
(a) in a way that denies the second person the economic or financial autonomy the second person would have had but for that behaviour; or
(b) by withholding or threatening to withhold the financial support necessary for meeting the reasonable living expenses of the second person or the second person’s child, if the second person is entirely or predominantly dependent on the first person for financial support to meet those living expenses.29
Economic abuse can involve a person taking control of all finances, restricting a person from working or spending money or denying access to money (including their own), misusing responsibilities as power of attorney, accessing and using a person’s bank account without their permission, threatening or demanding money from a person, or providing only small amounts of money for a person or family to live on. Economic abuse can also involve exploitation which does not directly involve money, for example taking out a loan under the name of a person without their permission, or threatening to have essential services, such as electricity or gas, disconnected, or leaving victims with unpaid bills for these services. Making significant financial decisions without consulting the victim, selling their possessions, or destroying property can constitute economic abuse. Incurring debts under a victim’s name or on shared property or rental houses, where debt can be incurred by the victim to make repairs.
Threats
Threatening behaviours can cross the spectrum of all other types of family violence, including threats to hurt victims, children or pets, threats to use a weapon, or the withhold a person’s access to financial, social, and spiritual or social support. Threatening behaviours can be seen as a type of emotional or psychological abuse that rely on other types of family violence as a component of the behavior. While in some cases threats may be experienced as other types of abuse (e.g. physical or sexual abuse), they may also be more generally understood as behaviours that are threatening. In some circumstances, where another abuse has occurred, the threat may relate to the abuse re-occurring if the victim does not act or change their behavior as required by the perpetrator. Threats may include the use of weapons or objects as weapons to increase fear. Threats may be verbal or non-verbal.
Coercion
Coercive controlling violence is an ongoing pattern of use of threat, force, emotional abuse and other coercive means to unilaterally dominate a person and induce fear, submission and compliance in them. Its focus is on control, and does not always involve physical harm. Coercion may be experienced by a victim survivor as emotional abuse, however it has an added dimension of domination and control. Controlling behaviours include obsessive jealousy, and can manifest in social and familial isolation and stalking (including monitoring of a victims telecommunication or online social media activities). Examples of these behaviours include dictating what a victim does, who they see or talk to, or where they go This includes preventing a victim from making or retaining friends, communication with family or access to money or essentials. This can include preventing a victim from going to work, not allowing them to express feelings or thoughts, not allowing privacy or forcing them to eat or drink, or limiting access to food or drink.
Exposure to family violence (child)
When defining family violence, the FVPA specifically includes “behaviour by a person that causes a child to hear or witness, or otherwise be exposed to the effects of” family violence.30 The category of ‘exposure to family violence’ therefore specifically applies to children and young people who have indirectly been subjected to family violence. This can include witnessing a family violence incident or the aftermath of an incident (for example, a parent with injuries or broken furniture), protecting family members, pets or others during a family violence incident, or feeling unsafe within the home because of family violence.31
Exposure to violence includes direct and indirect impact of family violence and the effects on physical environment or the control of other adult or child family members. Risk of harm may be higher if a perpetrator is targeting certain children, particularly non-biological children or young people in the family. Exposure may be direct and include use of coercive control over the child or young person or physical or sexual violence.
Unborn children can also be impacted by family violence, which may cause premature birth, low birth weight, foetal injury and foetal death. Unborn children may also be impacted by actions taken against their mother, including denial of access to food and antenatal health services. In the Children, Youth and Families Act 2005 (Vic)32, a person may make a report if there is significant concern for the wellbeing of an unborn child.
A child or young person can experience all of the family violence risk factors that an adult can experience. A child or young person may also experience violence when trying to intervene in violence being used against another family member, or through the undermining of a child-parent relationship from a perpetrator, and the subsequent impact on parenting and the child-parent bond. A child or young person who is using aggressive language or behavior may indicate they are being exposed to or are directly experiencing family violence.
Defining family member
Under the FVPA, a family member includes any person who is or has been a spouse or domestic partner, an intimate partner, a relative, a child or young person who normally or regularly resides (or has resided) with the relevant person, or a child of a person who has or has had an intimate personal relationship with the relevant person. For the purposes of the FVPA, a relationship may be considered an intimate personal relationship whether or not it is sexual in nature.
| Extended definition of family member |
|---|
|
In the FVPA, the term ‘family member’ is defined broadly to include intimate partners, relatives and ‘familial-like’ relationships. Section 3 of the FVPA sets out a range of criteria to assist with determining whether it is reasonable to describe a relationship as ‘like a family member’. The criteria include examining the nature of social and emotional ties, living arrangements, the duration of the relationships and financial dependence or interdependence between the parties.36 Perpetrators of family violence may therefore include not only conventional family relationships, but also caregivers, co-residents and members of extended kinship networks. It was noted by the RCFV that the extended definition of family member may not be widely known by family violence first responders and service providers. As such, incidents of abuse which meet the criteria for family violence may go unrecognised. This not only impacts the data collected on people affected by family violence, but also the availability of services to them after reporting abuse. |
Challenges in current data collection practices
Significant work is underway as part of the family violence reforms to strengthen workforce capacity to identify and respond to family violence. However historically, identifying family violence has not been a core business function of many agencies and services providers who may routinely interact with victims and perpetrators. In addition, staff in mainstream services, such as schools, hospitals and services for the elderly, may not have sufficient training to feel confident to identify family violence, or to recognise family violence that is not intimate partner violence. This can mean a lack of systems and processes to support consistent data collection on family violence. For example, at the time of the RCFV it was noted that the data collected in schools regarding student support services did not routinely flag information as family violence related, and such information would have to be extracted from key words used in case notes.33
In recent years, there has been a push for agencies and services to collect family violence as a ‘flag’, which indicates if a case or record is related to family violence. While this practice is an improvement in collecting information on family violence, it can limit the detail of information collected. How agencies define family violence may be unique to their own internal mandates, funding arrangements and operational purpose, meaning that a family violence flag may not be used consistently across agencies.
Existing standards
Types of family violence
There are limited existing administrative data standards in Australia which are used to record types of violence or abuse in the context of a family violence incident. The national minimum data set for Child Protection records abuse and neglect type (METeOR identifier: 455487) for the most serious type of abuse or neglect that has caused, or is likely to cause, injury or harm to a child or young person. Response options for this standard are:34
| Value | Meaning |
|---|---|
| 1 | Physical abuse |
| 2 | Sexual abuse |
| 3 | Emotional abuse |
| 4 | Neglect |
While these responses overlap with many behaviours relevant to family violence, this standard was developed for use specifically in a child protection context, and the scope of the responses is therefore not wide enough to capture all behaviours which meet the definition of family violence.
The Family Services Integrated Reports and Information System (IRIS) Data Dictionary developed by DHHS for the Child Family Information Referral and Support Teams (ChildFIRST) and Integrated Family Services Program contains a standard for recording family violence type, where the options listed include physical abuse, emotional or psychological abuse, economic abuse, and youth family violence to record current or historical family violence experienced by members of a family.35 While the first three options refer to a specific kind of abusive behaviour, ‘youth family violence’ is an option used to capture family violence behaviours which are perpetrated by a young person within the family context.
Relationship types
There are also few existing administrative data standards in Australia which are used to record types of relationships in the context of a family violence incident. The Disability Services National Minimum Data Set includes a data item (METeOR identifier: 680219) for recording the interpersonal relationship of carer to care recipient, however the response values for this data item are limited, and it is designed to capture primarily adult relationships (for example, son-in-law, daughter-in-law).36
The Housing Assistance National Minimum Data Set includes a data item which collects the familial and non-familial relationship of each person in a given household to a designated person in that household (METeOR identifier: 609147). The response options for this data item are also limited, and do not collect familial information outside of spouse/partner and son/daughter.37
The National Coronial Information System (NCIS) has a robust data item concerning ‘perpetrator relationship to deceased’ in their data dictionary.38 This standard contains over 25 different response options for relationship type with accompanying data definitions. It is also uniquely hierarchically structured, so that in the event that more than one relationship category could apply to a perpetrator, coding can reflect the relationship with the highest interpersonal ranking.
Data collection standards for collecting information about family violence
This section introduces three data items to improve the consistency and quality of information collection about family violence. These items are:
- Type of family violence
- Type of relationship
- Role of party
The purpose of these data items is not to set standard definitions for family violence, which are established in the FVPA. Organisations looking for definitional information to support implementation should consult that FVPA, as well as materials develop as part of the family violence reform, including the MARAM framework.
When planning for implementation, government departments, agencies and service providers can consider how the data collection standards detailed here can be applied to or supplement existing data items, such as existing family violence flags. For example, a helpline may already collect some information on the types of violence or abuse that callers have experienced and the framework suggests that the response options for types of violence can be added to the existing data item, rather than creating a second data item.
Types of family violence
Family violence differs from other forms of violence because it is part of a pattern of behavior that controls or dominates the family member and causes that family member to feel fear for their safety or wellbeing or of another person. Data suggests that where physical violence occurs, other noncontact forms of family violence (emotional/psychological abuse, economic abuse, coercion or threats) are also likely to be present. As such, a single incident may not reflect the full range of types of family violence that have been experienced or used.
For this reason, organisations and professionals should recognise that the types of violence recorded at this data item may include those that have not been used in the specific incident that led a victim or perpetrator to seek support. This is particularly relevant if data entry is drawing on information that is gathered through completion of a family violence risk assessment, which includes a range of questions about a person’s historical experiences of family violence. The inclusion of historical information in a client’s administrative record may have implications for data analysis and reporting, in particular if analysis attempts to describe types of family violence that are experienced or used at a specific point in time.
It is recommended that when updating IT systems to include this data item, that the option to record multiple types of family violence is enabled. Collecting information on all forms of identified violence can help build the evidence base on the more concealed types of family violence, and encourage greater recognition of specific types of violence that may be over-represented in priority communities.
Development of the standard
The standard for recording types of family violence proposed within this framework mirrors the categories of violence described in the FVPA. These categories have been assessed for their alignment to the risk factors within the MARAM framework, as well as to existing categories used within the Personal Safety Survey, and the Victorian Population Health survey. This is intended to enable practitioners to draw on information collected through family violence risk assessment when recording data at this item, and will also support aggregation and analysis for research, evaluation and performance monitoring purposes.
Although specific types of family violence have been defined separately under ‘Defining family violence’ on page 26, the categories of emotional, psychological, spiritual and social abuse have been combined into a single response category due to the overlap that exists in their meanings. Child exposure to family violence is specifically identified by the FVPA as a type of family violence, and was therefore identified as a type of family violence which should be captured separately. However it is also important to acknowledge that children and young people are victim survivors in their own right, and that the range of types of family violence they experience should be recorded whenever possible.
Data item and response categories
| Forms of family violence identified or disclosed [select all that apply]
□ Physical |
Relationship between parties
Another important pieces of information that helps understand the nature of family violence is the relationship between the victim and the perpetrator.
Some services and agencies may have a narrowed focus on the different relationships involved in a family violence incident. As previously noted, services who report family violence data to a federal level funding source for specific service provision, for example, may only identify cases as family violence related where the parties involved are intimate partners, or where the victims are women and children. However, the FVPA adopts a broad definition of a family member and that definition is applied here.
The ‘relationship between parties’ asks organisations to record the relationship between two parties involved in family violence. It is important for all organisations to record all familial-like relationships involved in incidents of violence or abuse. This will ensure that data collected in Victoria will contain sufficient detail to identify when incidents of abuse occur within a family or familial-like relationships.
As previously noted in the ‘Types of family violence’ data item, the ongoing nature of family violence may mean that family violence may continue even while relationship status changes. For example, the period of time immediately after a victim leaves a violent intimate partner relationship is acknowledged as a high risk period, and as such, a change in relationship status can signal that a person is at increased risk. It is recommended therefore that the type of family relationship between the victim and the perpetrator is identified and recorded in each instance that a client discloses family violence, including where the relationship is an ‘ex-‘ relationship. Where IT infrastructure allows, it is recommended that the sub-category response options detailed below are used to capture the most detailed information about the relationship involved in the incident.
Development of the standard
The standard for collecting relationship between parties was heavily influenced by the standard used by the NCIS, and by consultation with stakeholders. The resulting data collection standard used in this framework contains both broad and sub-category response options to accommodate agencies and service providers who may have limited capacity to collect against a large list of possible responses. The sub-category response option list has been expanded from what is used by the NCIS to capture more detail about the familial and familial-like relationships involved in family violence. The standard in this framework omits all strictly non-familial relationships (for example, strangers) as these relationships fall outside of the scope of family violence. Data collectors and custodians may however choose to add such response options if they are seeking to capture information on relationships in a broader context than just family violence.
Data item and response categories
What is the party’s relationship to the victim/perpetrator?
| □ Current partner | □ Spouse □ De facto □ Girlfriend/boyfriend/partner |
| □ Former partner | □ Separated/divorced spouse □ Ex-de facto □ Ex-girlfriend/boyfriend/partner |
| □ Parent / Gaurdian |
□ Parent (biological/adoptive) □ Foster parent/guardian □ Step-parent/de facto of parent □ Partner of parent |
| □ Child | □ Child (biological/adoptive) □ Foster child/child cared for □ Step-child □ Child of partner |
| □ Sibling | □ Sibling (biological/adoptive) □ Half-sibling □ Step-sibling □ Foster-sibling |
| □ Other family | □ Grandparent □ Grandchild □ Aunt/uncle □ Niece/nephew □ Cousin □ Child in-law □ Parent in-law □ Sibling in-law □ Other (other family) |
| □ Familial-like | □ Kinship relationship □ Family of choice □ Formal/informal carer □ Person receiving care □ Co-resident □ Other familial-like relationship |
| Guide for use of responses |
|---|
|
Parent (biological/adoptive): This category should also be used to record same sex parents, or parents who have used donor assisted conception or surrogacy. Step-parent/defacto of parent, foster-parent, step-sibling and foster sibling: These categories should also be used to record parents/guardians and siblings who could be considered as ‘ex’. Child (biological/adoptive): This category should also be used to record children of same sex parents, or children from donor assisted conception or surrogacy. Grandparent, Grandchild, Aunt/uncle, Niece/nephew, Cousin: These categories include biological, adoptive and step relatives, and should also include relatives that may be considered ‘ex’. Kinship relationship: A cultural recognition that the relationship was ‘like family’ in the relevant person’s culture or community. In regards to Aboriginal communities, the kinship system is complex and determines how people relate to each other and their roles, responsibilities and obligations in relation to one another, ceremonial business and land.39 Family of choice: People with an LGBTI identity may establish a ‘family of choice’, which is comprised of individuals who are not necessarily biologically related but act as a chosen family for the individual. People may create a family of choice for many reasons including discrimination and rejection from their family of origin, and finding more in common with people who know what it is like to be part of a marginalised group.40 It should also include relationships that could be considered ‘ex-‘. |
Use with role of party data item
The relationship data item should be completed from the perspective of the client whose case record is being completed. For the purpose of analysis, relationship data can also be combined with the ‘role of party item’, as well as detail on age, gender and LGBTI identification, to provide more detail on the direction and nature of the relationship. This allocation of specific roles and relationships by family violence is more viable in sophisticated IT systems that support the creation of case records that are distinct from a client record, and that are able to be linked to other case records. This may be particularly relevant in cases that involve multiple victims or perpetrators.
Multiple victims or multiple perpetrators
Family violence events may sometimes involve more than one perpetrator or more than one victim, for instance, where an adolescent uses violence against their mother and their sibling. To accommodate for this complexity, organisations should consider how their data can be structured to capture relationship information between all parties involved in an incident. A best practice approach would be to create a unique case record for each client that enables each relationship and role of party to be recorded, acknowledging that not all IT systems support the grouping of client records into family groups.
Multiple relationship types
The response options above are structured in a hierarchical manner. Although a relationship between two parties may fall into more than one of the below categories, for clarity in the data it is recommended that only one relationship type is recorded between two parties at a single point in time (noting that the relationship status may change over time). The data item selected should represent the relationship at the time of recording. In the event that the relationship could fall into more than one category, the relationship with the highest interpersonal ranking should be selected. For example, if the victim of family violence was a person receiving care and the perpetrator’s biological child, ‘child (biological or adoptive)’ should be selected as the type of relationship.
Role of party
The role of a person during a family violence incident is often not recorded by services outside of police and court systems, where it is necessary to determine who is the perpetrator/respondent or victim/applicant. There are many service entry points which capture information about both victims and perpetrators of family violence, but it is not usually identified in data whether the client is an alleged victim or perpetrator.
As noted in the ‘Terminology’ section of the framework, there are a variety of terms used to differentiate between victims and perpetrators, and no single term will be appropriate for all services. For example, the term perpetrator is not often associated with adolescents who use violence in the home, as it is viewed as stigmatising and does not acknowledge the necessary developmental needs of the adolescent. Services who provide Adolescent Family Violence programs therefore may choose to record their client’s role within a family violence incident as ‘adolescent who uses violence’.
The role of party data item is relevant to a specific family violence incident, as it asks organisations to identify the role of a person during a family violence incident at a given point in time. For this reason, it must be acknowledged that the role of the party may change, which is particularly relevant for adolescents who use violence in the home. The role of party is ideally recorded on a client’s case record, which includes data relevant to a specific incident, as opposed to a more generic client record which holds general demographic data items.
This data item may not always be appropriate to collect directly from a person who was involved in a family violence incident, and organisations need to be cognisant of the challenges involved in identifying the predominant aggressor (discussed below). The ‘unable to be identified’ category has been included to help manage potential misidentification, by providing an alternative option. Use of this category will also assist in generating evidence on the extent to which identification of the role of a party is difficult.
Data item and response categories
| Role during family violence incident:
□ Victim |
Perpetrator/predominant aggressor and misidentification of the role of party
Some perpetrators of family violence report being victim survivors. A perpetrator can overtly present themselves as the victim of the violence to manipulate services, including police, to misidentify the real victim as a perpetrator. Presenting in this way is also consistent with ‘victim stance’ thinking that many perpetrators adopt to justify and excuse their behaviour. Perpetrators may also aim to convince service providers that they are the victim survivor, or use a range of behaviours to avoid or deflect their responsibility for using family violence.
Misidentification may occur where a victim survivor uses self-defence or violent resistance during an incident or series of incidents of family violence. Police or other professionals may misidentify a predominant aggressor (perpetrator) due to misinterpretation of the behaviour or presentation of a victim survivor.
Misidentification may also occur when a perpetrator:
- falsely accuses a victim survivor of using violence, or misrepresents their self-defence as evidence of violence
- cites substance abuse by the victim survivor as evidence to support their claim they are a perpetrator
- undermine a victim survivors presentation or behaviour as resulting from mental illness, or misrepresenting a victim survivor’s disability as drunkenness or being drug affected, minimising their opportunity to have their voice heard. This could be an example of a deliberate misrepresentation of a victim survivor which exacerbates or leverages discriminatory attitudes commonly held in the community about people with, for example, disability or mental illness
This includes where a victim may not be able to communicate effectively with the police or service provider (due to trauma or from pre-existing communication barriers), may be injured, in shock or distraught as a result of the violence, or may be calm or assertive, or may fear reprisals from showing their reaction from the violence.
The inclusion of the ‘unable to be determined’ category is also intended to assist in reducing misidentification within data, however is ideally used as a temporary category. Where a professional is ‘unable to determine’ if an individual is a victim or a perpetrator, they should seek secondary consultation with a specialist family violence service or other professional with authorisation as a Risk Assessment Entity to undertake further enquiry into the identity of ‘alleged perpetrators’ under the Family Violence Information Sharing Scheme. The MARAM Framework Practice Guidance provides practice considerations to assist specialist practitioners in determining identity of a perpetrator/predominant aggressor and a victim survivor.
23 Family Violence Protection Act 2008 (Vic) s.5(1).
24 Australian Institute of Family Studies (AIFS) 2015, What is child abuse and neglect?, viewed 13 June 2018,
https://aifs.gov.au/cfca/publications/what-is-child-abuse-and-neglect
25 Victorian Centres Against Sexual Assault (CASA Forum) 2015, What is family violence? [factsheet], Springvale Monash Legal Service Inc, viewed 20 June 2018, www.casa.org.au/survivors-and-friends/family-violence
26 ABS 2014, 4102.0 Australian Social Trends, viewed 13 June 2018, www.abs.gov.au/ausstats/abs@.nsf/Lookup/4102.0main+features602014
27 Senior Rights Victoria, Social Abuse, viewed 13 June 2018, http://seniorsrights.org.au/your-rights/social-abuse/
28 Department of Communities, Child Safety and Disability Services (QLD), Domestic and Family Violence and Its Relationship to Child Protection [Practice paper, October 2012], viewed 6 June 2018, www.dfvbenchbook.aija.org.au/understanding-domestic-and-familyviolence/cultural-and-spiritual-abuse/kl
29 Family Violence Protection Act 2008 (Vic) s.6.
30 Family Violence Protection Act 2008 (Vic) s.1(b).
31 AIFS 2015, What is child abuse and neglect? viewed 13 June 2018, https://aifs.gov.au/cfca/publications/what-is-child-abuse-andneglect
32 Children, Youth and Families Act 2005 (Vic).
33 RCFV 2016, Volume 2 Report and recommendations, p.120.
34 AIHW Metadata Online Registry, Child – primary type of abuse or neglect, code N[N], viewed 12 June 2018,
http://meteor.aihw.gov.au/content/index.phtml/itemld/455487
35 DHHS 2013, Family Services IRIS Data Dictionary, viewed 13 June 2018, providers. dhhs.vic.gov.au/sites/dhhsproviders/files/2017-06/Family-services-IRIS-data-dictionary.docx
36 AIHW Metadata Online Registry, Informal carer – relationship to care recipient, interpersonal code N[N], viewed 12 June 2018,
http://meteor.aihw.gov.au/content/index.phtml/itemld/680219
37 AIHW Metadata Online Registry, Person – relationship to household reference person, code N, viewed 12 June 2018,
http://meteor.aihw.gov.au/content/index.phtml/itemld/609147
38 National Coronial Information System 2017, Data Dictionary for the National Coronial Information System Version 3 July 2010 [Revised 13 June 2017], viewed 13 June 2018, www.ncis.org.au/about-the-data/system-manuals/
39 Central Land Council, Kinship and skin names, viewed 20 June 2018, www.clc.org.au/index.php?/
40 QLife 2016, Families: A QLife Guide for Health Professionals, viewed 13 June 2018, https://qlife.org.au/qlife-guides/
Data collection standards - Children and young people
Discusses improvements which can be made to data collection practices to improve the quality of administrative data concerning children and young people affected by family violence.
Children and young people were recognised through framework consultations as a key data gap concerning experiences of family violence in Victoria. The RCFV heard that children and young people are often ‘silent victims’ of family violence because services have primarily focused on the safety and wellbeing of women within the context of intimate partner violence. Administrative data collection practices have often grouped young victims into case records belonging to a parent or guardian, rather than recording children and young people as victim survivors in their own right. This includes unborn children who can also be impacted by family violence.
As a result, information collected on children and young people impacted by family violence is limited. The RCFV also heard that many incidents of adolescent violence in the home (AVITH) are not captured in data for a variety of reasons, including under-reporting. This section of the framework discusses improvements which can be made to data collection practices to improve the quality of administrative data concerning children and young people affected by family violence.
Terminology and definitions
There are many terms which can be used to describe children and young people, including juveniles, adolescents, and youths. While these are all acceptable terms, this section will primarily use the term ‘children and young people’, which is consistent with language used in the RCFV and encompasses all individuals aged up to and including 25 years old.
The age used to define children and young people varies across agencies and service providers. In Australia, the age of 18 years is used to broadly distinguish between children and adults. The RCFV used the term ‘child’ to refer to people under the age of 18 years, and ‘young people’ to describe individuals up to and including 25 years of age.41 Specific organisations may break down ages into different categories for their own internal reporting purposes, and the framework does not advise how organisations should define and describe children and young people. Rather, it encourages the collection of disaggregated data surrounding family violence to improve the detail of information available concerning children and young people who experience family violence, including unborn children.
| Child abuse and family violence |
|---|
|
The Department of Health and Human Services Child Protection manual defines child abuse as “any action, or lack of action, that significantly harms the child’s physical, psychological or emotional health and development. Child abuse can occur within a single incident or on multiple occasions and is categorised in the following manner: Neglect is defined in the Child Protection manual as “failure to provide the child with an adequate standard of nutrition, medical care, clothing, shelter or supervision to the extent where the health or development of the child is significantly impaired or placed at risk. A child is neglected if they are abandoned or left uncared for over unreasonable periods of time that is inconsistent with their age, stage and development.”43 The Australian Institute of Family Studies (AIFS) similarly defines child abuse and neglect as ”any actions of commission or omission by a parent, caregiver or other adult that results in harm, potential for harm, or the threat of harm to a child... even if the harm is unintentional”.44 Five subtypes of harm are further broken by the AIFS to include physical abuse, emotional maltreatment, neglect, sexual abuse and witnessing family violence.45 The Children Youth and Families Act 2005 (Vic) also enables consideration of the pattern and history of harm and the impacts on a child’s safety, stability and development. There is an overwhelming body of evidence which indicates that chronic neglect, abuse and family violence are harmful and have a cumulative and detrimental effect on a child’s development. The Children Youth and Families Act 2005 (Vic) acknowledges the impact of child abuse and neglect on unborn children. Within the act, a person may make a report if there is significant concern for the wellbeing of an unborn child. The definition of family violence provided under the FVPA does not expressly capture all instances of child abuse so defined (in particular, acts of unintentional neglect, or actions committed by a person who does not have a familial-like relationship with a child), but there is overlap between the two concepts. This framework acknowledges that child abuse and family violence are not discrete concepts, and definitions for both of these may vary across states, departments and services. As such this framework does not provide advice about how to differentiate between child abuse and family violence. |
Family violence and children and young people
Family violence can have serious impacts on the health, development and wellbeing of infants, children and young people. Despite these concerns, currently there is a significant gap in existing survey and administrative data about children and young people who experience family violence. Recognising children and young people who experience family violence as victim survivors in their own right is an important part of addressing this gap.
Prevalence
Evidence suggests that family violence experienced by children and young people often goes unreported, which makes it difficult to assess the full extent to which they are affected by family violence.46 This was noted by the RCFV, and more recently by the AIHW in their 2018 report on family, domestic and sexual violence.47, 48 Despite these limitations, survey and administrative data indicates that many children and young people in Victoria are direct and indirect victimsi of family violence and that some may also use violence in the home.
Information published by the Crime Statistics Agency (CSA) in the 2016-17 iteration of the Victorian Family Violence Database (FVDB) indicated that children were recorded by Victoria Police as being present at 31% of all family incidents in the 2016-17 financial year. People under the age of 18 years made up 10% of all recorded affected family members and 6.6% of all other parties in that same financial year.49 The 2016 Personal Safety Survey (PSS) found that nationally, for 1 in 2 women (50%) who experienced violence from a current partner, and 2 in 3 women (68%) who experienced violence from a former partner, children had also seen or heard the violence.50
Contributing circumstances and specific presentations of family violence risk
Children and young people are victim survivors in their own right, and experience many forms of family violence including physical, emotional, and sexual abuse. In addition, section 1(b) of the Family Violence Protection Act 2008 (Vic) (FVPA) describes that an incident may also constitute family violence if “behaviour by a person... causes a child to hear or witness, or otherwise be exposed to the effects of” family violence (including physical, sexual or emotional abuse).51 These experiences are typically referred to as ‘secondary’ or ‘indirect’ family violence victimisation, and the FVPA clearly articulates such experiences as a distinct type of family violence affecting children and young people. Children may therefore be exposed to a multitude of experiences of family violence outside the types of behaviour which are often associated with it.
Children can experience all risk factors that can be experienced by an adult and there are additional recognised risk factors specific to children or their circumstances outlined in the MARAM Framework and practice guidance. These experiences of risk factors can present in a range of ways and can include:52
- direct witnessing of or intervening in incidents of violence against a family member53
- indirect knowledge of incidents against a loved one including being aware of threats of abuse,
- physical injuries, property damage, or psychological harm to others54
- being subjected to indirect physical harm (for example, a mother being struck while holding a baby)55
- having to be responsible for the care and safety of pets and family members56
- being made to feel they are responsible for the violence57
- loss of housing, treasured possessions or a sense of security because of violence58
- experiencing disruptions to schooling including prolonged absences or attending multiple new schools in a short space of time59
- feeling unable to bring friends home or being marginalised because of a perpetrator’s controlling or unpredictable behaviour60
Specific circumstances and presentations of Adolescent family violence in the home and in intimate partner relationships
The RCFV heard that children and young people are not only victims of family violence, but also sometimes use violence against their parents, siblings, girlfriends and boyfriends, and other family members. There is no one determinant of adolescent family violence, and it is believed to be the product of a range of multifaceted and interconnected dynamics.61 Research indicates that adolescents who use family violence may have experienced family violence themselves as children, and their behaviour is a continuation of intergenerational violence.62 In particular, Child & Family Service Ballarat Inc. reported in their submission to the RCFV that 80% of the adolescents who attended their AFV program reported experiencing violence in the home themselves, predominantly perpetrated by a father or stepfather.63 Victims of violence used by adolescents include parents, siblings, grandparents and family pets.64
Adolescents can also use violence in their intimate relationships, and this is recognised as a unique presentation of family violence risk. The RCFV noted that there is under-reporting and underrecognition of adolescent family violence, which contributes to an absence of administrative data available on the subject.
Additionally, much of the existing administrative data in Victoria concerning adolescent family violence comes from information recorded by police responding to family violence incidents, however this data does not fully capture the extent of this issue. The RCFV noted that AVITH is likely to be underreported to police by parents for a variety of reasons:65
- feelings of parental guilt, self-blame, shame and denial
- minimisation of abuse (for example, excusing behaviour as inherent traits or learnt behaviour)
- fear of how the adolescent might react upon discovering a report to police
- fear that their child may get a criminal record if the violence is reported
The limited options that police have to respond to AVITH may also contribute to a reluctance for parents or carers to report an adolescent’s behaviour to police. In their 2018-2023 strategy for family violence, sexual offences and child abuse, Victoria Police noted that at present “police options to respond to family violence are limited in cases involving child or youth perpetrators”.66 Family Violence Safety Notices and holding powers cannot be used on children and young people who use family violence, due to concerns about the negative impact of such actions on young people. Additionally, children, young people and adolescents who use family violence are recognised to have complex needs, including increased association with mental illness, acquired brain injuries, the use of drugs and alcohol, and past exposure to family violence.67
Under-reporting and barriers to accessing services
As with most instances of family violence, under-reporting was recognised by the RCFV to play a major role in the absence of data surrounding children and young people and their experience with family violence.68 Children and young people are especially vulnerable to being subjected to unreported violence, as perpetrators of incidents against children and young people are often their parents or a person whom they depend on for care.69 In such circumstances children and young people may be reluctant or unable to report abuse against their parent or guardian, and they may not recognise that the behaviour is unusual or constitutes violence. Therefore, staff in mainstream services, including registered doctors, nurses, midwives, early childhood teachers, school teachers and principals can play an important role in the identification and early intervention of children and young people who are experiencing family violence.
The RCFV noted that children and young people may face additional barriers to accessing family violence services or reporting incidents. It was noted that children and young people are less likely than other age groups to seek help, and that this reluctance may be a consequence of “confusion, poor self-esteem and lack of accessible information”.70
Effects of family violence on children and young people
Not all children and young people exposed to family violence are affected in the same way. For some, the effects of family violence may be chronic and debilitating, whereas others may have less adverse outcomes. A range of positive and negative factors may impact a child or young person’s resilience or vulnerability to family violence.71 It should therefore not be assumed that a child or young person will fare worse than children who have not experienced family violence or that they will become perpetrators themselves. However, the RCFV noted that family violence has the potential to cause serious impacts on the health and wellbeing of infants, children and young people. Evidence about the severity of the impacts of family violence on children and young people affirms the importance of recognising and responding to children and young people as victim-survivors in their own right. Some of the effects of violence against children and young people are noted below.
- Intergenerational transmission of abuse and neglect: Although most survivors of child maltreatment do not go on to maltreat their own children, evidence suggests that those who were abused or neglected as children and young people are at an increased risk of intergenerational abuse, neglect, re-victimisation or perpetration of family violence.72
- Complex trauma: This is a term which refers to the “multiple and interacting symptoms, disorders and the broad range of cognitive, affective and behavioural outcomes associated with prolonged and cumulative trauma”.73
- Re-victimisation: Research suggests that adults, particularly women who were child victims of abuse or neglect, are at a risk of re-victimisation later in life.74 Results from the 2016 PSS indicated that children who witnessed partner violence against their parents were 2-4 times as likely to experience partner violence as adults than children who had not.75
- Attachment and interpersonal relationship problems: Trauma caused by family violence can result in damage to a child or young person’s brain development, reducing their capacity to self-regulate their behaviour. Coupled with learned adaptive responses to trauma, children and young people may develop patterned behaviours which impact their attention, memory, sense of identity and their relationships.76 This, in combination with poor early childhood attachments may initiate a lifelong trajectory of interpersonal difficulties.77
- Developmental impacts: Research has shown that exposure to family violence, especially in the early years can have a significant impact on children’s development, largely because it disrupts attachment, over-develops regions of the brain involved with anxiety and fear responses and limits children’s opportunities for interaction and play-based learning.78 Family violence can also affect a child or young person’s development via an impact on school attendance, housing security, social connectedness and educational or social factors.79
- Youth suicide: Research suggests that there is a link between youth suicide and abuse, with some research finding that all forms of child maltreatment were associated with adolescent suicidal ideation and suicide attempts, in particular child sexual abuse and emotional abuse.80
- Aggression, violence and criminal activity: Research suggests that physical abuse and exposure to family violence are the most consistent predictors of youth violence. A study in the US found that abused and neglected children were 11 times more likely to be arrested for criminal behaviour in adolescence.81
- Impact on unborn children: family violence against pregnant women may cause premature birth, low birth weight, foetal injury and foetal death. Unborn children may also be impacted by actions taken against their mother, including denial of access to food and antenatal health services.
Why do we need to collect information on children and young people?
There is a lack of data concerning the experiences of children and young people as both victims and people who use family violence. Currently there is very limited evidence collected in both surveys and administrative data which can be used to make informed decisions about service use, responsive intervention strategies and to understand the overall experiences of family violence faced by children and young people. The collection of high quality administrative data concerning children and young people presents an opportunity to improve the evidence base on children and young people impacted by family violence.
Limited identification of child victims of family violence in data
A key theme emerging from the RCFV was that children and young people experiencing family violence should be recognised as victim-survivors in their own right. In administrative data, mothers or caregivers are often recorded as a primary victim of family violence, and details about affected children and young people are either not collected, or exist in case notes and therefore cannot be suitably used for data analysis. This approach not only de-values the impact of family violence on a child or young person, but it also compromises the quality of administrative data collected about the experiences of children and young people affected by family violence. By missing the opportunity to collect information on children and young people who present at a service with a parent or guardian, it is difficult to know the extent, nature and outcomes of family violence on this population. It will also be difficult to consider important demographic details about these victims, including whether they belong to other priority communities, and to track the trajectory of these individuals through service data over time.
Data collected on children and young people as victims is more often picked up by child-specific services such as education, child protection and health care services. As data systems set up for these services may not be specifically designed to capture information on family violence, this will contribute to data gaps. Although the FVPA specifically identifies children and young people who witness or are otherwise affected by family violence as victims in their own right, there is a risk that non-specialist family violence agencies and services will make their own assessments about whether a child or young person is or is not a victim of violence and abuse, particularly if staff have not been trained in identifying family violence. This may contribute to an under-representation of children and young people who experience family violence.
Gaps in information
There are many noted gaps in knowledge surrounding children and young people’s experiences with family violence, and at the most basic level “there is little to no research about understanding the impact of family violence from the young child’s perspective”.82 As details of children’s experiences are often bundled with the experiences of adult victims of family violence, disaggregated data concerning children and young people affected by family violence is rarely collected. As a result there are noted gaps in information on:
- the prevalence of family violence affecting children and young people83
- the extent of violence occurring between siblings or other familial relationships outside of parents and intimate partners84
- the long-term effects and cumulative harm of direct and indirect exposure to family violence on children and young people85
- the experiences of children and young people from other priority communities including children with disability or mental illness, Aboriginal and Torres Strait Islander children, children from culturally and linguistically diverse backgrounds or LGBTI children and young people86
- details surrounding children and young people who use family violence, including:87
- the nature and extent of this type of family violence
- the impact that prior exposure to family violence as a victim-survivor has on children and young people who go on to use violence themselves
- the availability and efficacy of services available for children and young people who use family violence
Challenges in current data collection practices
There are a number of challenges which impact the ability to collect information on children and young people as unique individuals when they present for service with a parent, including IT restrictions and lack of training and education about proper data collection practices. Of significant concern is that detailed information about children and young people affected by family violence can be limited in administrative family violence data if a service provider or agency only captures information on adult victims of violence. This may occur if existing IT infrastructure one supports one client to be attached to a case file or record in their data management system, limiting organisations’ capacity to record detailed client information on multiple people affected by the same family violence event. It may also occur if organisations are not specifically resourced to provide family violence services to children and young people. The RCFV noted for example that details about children and young people captured in specialist family violence service data are sometimes lost, where children are counted as ‘add-ons’ to their mothers.88 Additionally, due to the broad range of entry points where children and young people may be captured, these individuals may not be accurately recognised as victims of family violence.
Data collection standards for collecting information on children and young people
While this data framework does not introduce additional data standards in relation to children and young people, there are specific issues organisations should be aware of when collecting information on family violence. This section includes advice on the complexities of collecting information from children and young people, and also on specific considerations when applying the family violence data items to this priority community.
Collecting data from children and young people
It is important to collect information directly from a child or young person regarding their experiences with family violence whenever possible and appropriate.89 Respecting a child or young person’s right to have a say and be heard is important in acknowledging their role as a victim who has experienced family violence, even in circumstances where the violence was indirect. Gathering information directly from the victim will also provide insight on how children and young people uniquely experience family violence and will allow them to self-identify with the other priority communities discussed in this framework.
However, collecting information from children and young people that accurately and authentically reflects their experience can be difficult. As highlighted in the National Health and Medical Research Council’s National Statement on Ethical Conduct in Human Research, different levels of maturity and the corresponding capacity to be involved in decision making need to be considered when working with children and young people.90 Although this report concerns data collection in research, the principles can be applied to an administrative context. The Communities and Families Clearinghouse Australia released a practice sheet in 2011 which provides information on best practices for collecting information from children and young people. They note that services should be mindful of the following when looking to collect data directly from children:91
- Issues of privacy and confidentiality are especially significant when collecting information from or about children and young people. The recent introduction of the FVIS Scheme and the CIS Scheme impact privacy and confidentiality, and organisations should be clear about their obligations and authorisations under those schemes. Staff should also prepare for the possibility that a child or young person may disclose information which is subject to mandatory reporting or may be shared to assess or manage family violence risk or promote safety and wellbeing and ensure that the child or young person understands the limitations of privacy and confidentiality.
- Ethical issues: Care should be taken to factor in vulnerability and potential harm from collecting data directly from a child. Where a child or young person has been a victim of family violence, being asked to specifically recall incidents may cause distress to the child or young person. Data collection should therefore consider sympathetic methodologies, appropriate contexts, protocols and procedures which enable data collectors to prepare for and manage the potential for risk and re-traumatisation.92
- The age of the child: Collecting data directly from young children (6 years or under) which accurately reflects their experiences can be difficult, as they may not respond to traditional data collection methods (for example, surveys, interviews with strangers). Agencies and service providers should be aware of issues surrounding the age at which a child can consent to directly provide information which is captured in data.
- The method used to gather data should be considered depending on the age, developmental stage, skills and capabilities of a child. Written data collection for instance may not be appropriate if a child or young person is not comfortable with reading and writing. Similarly if a form is lengthy a child or young person may not have the attention span to complete the document. Non-traditional methods of data collection may make it easier to collect information and may make the process more effective for young children.
- Children and young people are more affected by leading questions and effort should be made to ensure that an interview is not intentionally or unintentionally leading a child or young person to certain answers. It should be made clear when working with children and young people that there are no correct or incorrect responses when speaking about their experiences.
- Children and young people given the option to have a parent present or not present: Wherever possible, children and young people should be given the option as to whether they would prefer to have a non-offending parent or guardian present when participating in interviews. A child’s answers to questions may vary depending on whether a parent or guardian is present. Data collectors should also be mindful in the context of family violence to consider the possibility that a parent or guardian is the perpetrator of abuse. In this circumstance it would not be appropriate to gather information from a child or young person with that parent or guardian present.
Collecting data on children and young people affected by family violence
Types of family violence
Research and evidence presented to the RCFV suggested that while children and younger people experience similar types of abuse as intimate partner violence, including physical and sexual violence,93 they can also witness or be exposed to the aftermath of violence against other family members. The FVPA classifies this type of exposure as a distinct kind of family violence, in acknowledgment of its impact on children and young people. However children and young people who are exposed to family violence should be treated as victims in their own right, rather than as bystanders, witnesses or secondary victims. This includes unborn children who can also be impacted by family violence.
Thus while the data collection framework currently includes ‘exposure’ as an item within the ‘type of family violence’ data item, it is expected that, over time, and as a result of work underway as part of the family violence reforms, organisations will be increasingly equipped to identify the types of family violence that children and young people experience through other categories. This may result in reduced use of the ‘exposure’ response, as it is increasingly acknowledged that an indirect experience of family violence may be described through other terms, for example as emotional abuse.
Relationship between parties
Unlike other victims of family violence, children and young people are more likely to be affected by family violence perpetrated by a family member who is not an intimate partner. Victoria Police data published by the CSA showed that in the financial year 2016-17, a parent was recorded as the other party in 63.6% of family incidents where the affected family member was under 18 years of age.94 Less information is currently known about other types of relationships where children are impacted by family violence, however this can include an adolescent who uses violence against siblings, as well violence in the context of adolescent intimate partner relationships. Information on the relationship between parties is therefore important to increase understanding of family violence involving children and young people and the family members who are most often associated with these events.
Role of party
When recording children or young people who present with their mothers or guardians as clients of a service, agencies and services are encouraged to record these children and young people separately as unique victims. These children and young people should also be classified as victims, and not ‘secondary victims’ or ‘indirect victims’, regardless of whether they experienced direct or indirect family violence. Recording children and young people under other terms discredits the impact that exposure to family violence can have on a child or young person.
Accurate identification of the role of the party is particularly relevant within the context of adolescent family violence. The RCFV determined that adolescents who use violence in the home should be recognised by the family violence system as different to adult-perpetrated family violence. The drivers behind adolescent family violence must be considered using a developmental lens, and with a recognition that language such as perpetrator is stigmatising. It is also likely that a young person using violence is a victim survivor of past or current family violence.
Training and resources
Blue Knot
The leading national organisation working to improve the lives of Australians who have experienced childhood trauma. This includes people who have experienced child abuse in all its forms, neglect, domestic violence in childhood and other adverse childhood events.
Website: www.blueknot.org.au
Phone: 02 8920 3611
Centre for Excellence in Child and Family Welfare
The peak body for nearly 100 child and family services in Victoria, providing training, advocacy and support to children, young people and families in Victoria.
Website: www.cfecfw.asn.au
Phone: 03 9614 1577
Kids Helpline
A free, private and confidential telephone and online counselling service specifically for young people between 5 and 25 years old in Australia.
Website: www.kidshelpline.com.au
Phone: 1800 55 1800
Maternal and Child Health Line
A state-wide telephone service available every day of the year for Victorian families with children from birth to school age. Maternal and child health nurses are available to provide information, support and guidance regarding a range of issues.
Website: www.education.vic.gov.au/childhood/parents/support/Pages/mchline.aspx
Phone: 13 22 29
Parentline
A confidential and anonymous phone counselling service for parents and carers of children and teenagers in Victoria. It offers counselling, information and support around a range of parenting issues.
Website: www.education.vic.gov.au/about/contact/pages/parentline.aspx
Phone: 13 22 89
41 RCFV 2016, Volume 2 Report and recommendations, p.102.
42 Child Protection Manual; cpmanual.vic.gov.au/glossary#h3_74
43 Child Protection Manual; cpmanual.vic.gov.au/glossary#h3_239
44 AIFS 2014, Who abuses children? viewed 13 June 2018, https://aifs.gov.au/cfca/publications/who-abuses-children
45 AIFS 2014, Effects of child abuse and neglect for children and adolescents, viewed 13 June 2018, https://aifs.gov.au/cfca/publications/who-abuses-children
46 RCFV 2016, Volume 2 Report and recommendations, p.103.
47 Ibid.
48 AIHW 2018, Family, domestic and sexual violence in Australia 2018, Cat. no. FDV 2, Canberra, p.42.
49 Crime Statistics Agency (CSA) 2017, Download data tables, viewed 13 June 2018, www.crimestatistics.vic.gov.au/family-violence-dataportal/download-data-tables
50 AIHW 2018, Family, domestic and sexual violence in Australia 2018, Cat. no. FDV 2, Canberra, p.71.
51 Family Violence Protection Act 2008 (Vic) s.1.
52 An indirect victim is any child or young person who was not directly targeted during a family violence incident, but was otherwise affected by it. This can include witnessing or overhearing violence, or being exposed to the aftermath of an incident (such as seeing broken furniture, injuries on loved ones, etc.)
53 Commission for Children and Young People 2015, Submission regarding Family Violence Issues, no. 790, viewed 22 June 2018,
www.rcfv.com.au/Submission-Review
54 Ibid.
55 RCFV 2016, Volume 2 Report and recommendations, p.106.
56 Ibid.
57 Ibid.
58 Ibid.
59 Ibid.
60 Ibid.
61 RCFV 2016, Volume 4 Report and recommendations, p.154.
62 RCFV 2016, Volume 4 Report and recommendations, p.156.
63 Child & Family Services Ballarat Inc., Submission to Royal Commission into Family Violence, no. 687, viewed 22 June 2018,
www.rcfv.com.au/Submission-Review
64 RCFV 2016, Volume 4 Report and recommendations, p.152.
65 Ibid.
66 Victoria Police 2018, Policing harm, upholding the right: Victoria Police strategy for family violence, sexual offences and child abuse
2018-2023, viewed 15 June 2018, www.police.vic.gov.au/retrievemedia.asp?Media_ID=134877
67 RCFV 2016, Volume 4 Report and recommendations, p.155.
68 RCFV 2016, Volume 2 Report and recommendations, p.103.
69 AIFS 2014, Who abuses children?, viewed 13 June 2018, https://aifs.gov.au/cfca/publications/who-abuses-children
70 RCFV 2016, Volume 2 Report and recommendations, p.138.
71 AIFS 2014, Effects of child abuse and neglect for children and adolescents, viewed 13 June 2018, https://aifs.gov.au/cfca/publications/effects-child-abuse-and-neglect-children-and-adolescents
72 AIFS 2014, Effects of child abuse and neglect for adult survivors, viewed 13 June 2018, https://aifs.gov.au/cfca/publications/effectschild-abuse-and-neglect-adult-survivors
73 AIFS 2014, Effects of child abuse and neglect for children and adolescents, viewed 13 June 2018,
https://aifs.gov.au/cfca/publications/effects-child-abuse-and-neglect-children-and-adolescents
74 AIFS 2014, Effects of child abuse and neglect for adult survivors, viewed 13 June 2018, https://aifs.gov.au/cfca/publications/effectschild-abuse-and-neglect-adult-survivors
75 ABS 2017, 4906.0 Personal Safety, Australia, 2016, viewed 14 June 2018, www.abs.gov.au/ausstats/abs@.nsf/mf/4906.0
76 Commission for Children and Young People 2015, Submission regarding Family Violence Issues, no. 790, viewed 22 June 2018,
www.rcfv.com.au/Submission-Review
77 AIFS 2014, Effects of child abuse and neglect for children and adolescents, viewed 15 June 2018,
https://aifs.gov.au/cfca/publications/effects-child-abuse-and-neglect-children-and-adolescents
78 DHHS 2012, Assessing children and young people experiencing family violence: A practice guide for family violence practitioners, viewed 15 June 2018, https://dhhs.vic.gov.au/assessing-children-and-young-people-experiencing-family-violence-practice-guide-familyviolence
79 Ibid.
80 Miller, A B, Esposito-Smythers, C, Welsmoore, J T & Renshaw, K D 2013, ‘The relation between child maltreatment and
suicidal behaviour: A systematic review and critical examination of the literature’, Clinical and Child and Family Psychology Review.
81 English, D, Wildom, C & Brandford, C 2004, ‘Another look at the effects of child abuse’, National Institute of Justice Journal, vol. 251, pp. 23-24.
82 RCFV 2016, Volume 2 Report and recommendations, p.103.
83 Ibid.
84 AIFS 2014, Who abuses children?, viewed 13 June 2018, https://aifs.gov.au/cfca/publications/who-abuses-children
85 AIHW 2018, Family, domestic and sexual violence in Australia 2018, Cat. no. FDV 2, Canberra, p.42.
86 RCFV 2016, Volume 2 Report and recommendations, p.112.
87 AIHW 2018, Family, domestic and sexual violence in Australia 2018, Cat. no. FDV 2, Canberra, p.30.
88 RCFV 2016, Volume 2 Report and recommendations, p.133.
89 AIFS 2011, Collecting data from parents and children for the purpose of evaluation, Communities and Family Clearinghouse Australia, viewed 15 June 2018, https://aifs.gov.au/cfca/publications/collecting-data-parents-and-children-purpose
90 NHMRC 1999, National Statement on Ethical Conduct in Research Involving Humans, viewed 6 June 2018,
www.nhmrc.gov.au/guidelines-publications/e35
91 AIFS 2011, Collecting data from parents and children for the purpose of evaluation, Communities and Family Clearinghouse Australia, viewed 15 June 2018, https://aifs.gov.au/cfca/publications/collecting-data-parents-and-children-purpose
92 Morris, A, Hegarty, K & Humphreys, C 2012, ‘Ethical and safe: Research with children about domestic violence’, Research Ethics, vol. 8, no. 2, p.136.
93 RCFV 2016, Volume 2 Report and recommendations, p.112.
94 CSA 2017, Download data tables, viewed 13 June 2018, www.crimestatistics.vic.gov.au/family-violence-data-portal/download-datatables
Data collection standards - Older people
Highlights the unique ways that family violence may be perpetrated against older people and the barriers they face when trying to report family violence.
Older people were recognised by the RCFV as a priority community affected by family violence. This section highlights the unique ways that family violence may be perpetrated against older people and the barriers they face when trying to report family violence. Improvements are suggested which can be made to data collection practices so that organisations can produce quality administrative data to provide information about the experiences and the impact that family violence has on older people in Victoria.
Terminology and definitions
There are many terms which can be used to describe older people, including elders, seniors and older persons. While these are all acceptable terms, this section will primarily use the term ‘older people’, which is consistent with language used by the RCFV and the AIHW.
| Elder abuse and family violence |
|---|
|
Violence or abuse against older people is more commonly discussed under the term ‘elder abuse’ rather than family violence. While both of these terms refer to a broad range of behaviours including physical, sexual, emotional, psychological or economic abuse, family violence specifies that this behaviour occurs within the context of a family or a familial-like relationship. While elder abuse and family violence are often discussed as discrete concepts, it should be noted that there is considerable overlap between these topics and they should not be viewed as mutually exclusive behaviours. An analysis of data concerning people seeking help from Seniors Rights Victoria found that approximately 90% of all alleged perpetrators of elder abuse were related to, or were in a de facto relationship with the older person.95 Similarly, carers who abuse older people can be family members, or could meet the definition of a family member under the extended definition of a family member in the Family Violence Protection Act 2008 (Vic). |
It should be noted that the age used to define older people varies greatly across different departments, services and studies. For many Australian Government departments, including the AIHW, the term ‘older people’ typically refers to individuals aged 65 years and over. Seniors Rights Victoria, however, typically assists people aged 60 years and over, or aged 45 years and over for Aboriginal and Torres Strait Islander people. Similarly, in Victoria people aged 60 years and over qualify to receive a senior’s card. Agencies may therefore define the age of older people as is necessary for their own internal purposes, and this framework does not suggest a standard age to be used. Rather, the framework suggests improvements which can be made to the overall quality of data collected concerning family violence, so that targeted analysis of populations, including older people, is possible.
According to data published by the AIHW, older people make up 15% of the Australian population and are a diverse group comprised of different socio-economic backgrounds, life experiences and cultures.96 While older people are often associated with poor health and functioning, Australia’s older population is typically living longer and healthier lives than previous generations.97 It should be noted however, that there is an overlap between age and disability, with over half of Victorians aged 65 years and over recorded as having a disability.98 This section of the framework focuses primarily on family violence issues affecting older people, while the ‘People with disabilities’ section addresses issues faced by people with disabilities. As there is considerable overlap between these communities, it is recommended that both sections are considered regarding issues affecting older people experiencing family violence.
Family violence and older people
Existing research on the abuse of older people in Australia indicates that this group should be considered as a priority in future responses to family violence. Elder abuse may take any form of presentation of family violence, however there is a higher prevalence of economic or financial abuse, often arising from a sense of entitlement from an adult child or carer, as well as social and service access isolation. Elder abuse can also resemble other forms of family violence, such as intimate partner violence, including sexual assault, which is experienced by older women.
Prevalence
It has been noted that limited information exists in Australia concerning the prevalence of family violence against older people. The RCFV estimated that elder abuse affects between 5-6% of the population of older people in Australia, however it is suspected that there may be considerable underreporting of incidents.99
In their 2016 research report on elder abuse, the Australian Institute of Family Studies (AIFS) noted that the growing population of older people in Australia adds additional concern to the prevalence of elder abuse.100 As Australia’s baby boomer population ages and the life expectancy in Australia increases, it is expected that the proportion of the population who are older adults will be higher than ever before.101 As such, there is a concern that rates of elder abuse will rise with the increased population. A growing ageing population reinforces the need to improve the detection of family violence directed at older people, and the availability of victim and perpetrator resources specifically tailored to this population.
Contributing circumstances and specific presentations of family violence risk
There are a number of contributing circumstances associated with older people which can impact the ways that family violence risk presents for this community. These include:
- having a cognitive impairment, diminished capacity or other disabilities102, 103
- recently having lost a spouse
- ongoing or resumed co-habitation with adult children
- being physically dependent on others
- living in poverty, or by contrast, having substantial resources104
- being socially isolated105
- living in rural, regional or remote communities which have reduced access to services106
- having a history of traumatic life events, including prior incidents of interpersonal and domestic violence107
In addition, structural inequality, discrimination and barriers, such as holding age-discriminatory views, including a lack of respect for older people or an opinion that older people are a burden are considered contributing to underlying drivers and intersect with drivers of family violence risk.108 Research and evidence presented to the RCFV suggested that older people can be at a heightened risk for psychological abuse and economic abuse, which includes having finances restricted or controlled by their abuser.109 When reliant on others for care, older people can also be victims of neglect, which includes withholding necessary medication or not receiving adequate personal hygiene care. This supports research by the AIFS, which found that psychological and financial abuse are the most common types of abuse reported by older people. Some studies suggest that “neglect could be as high as 20% among women in the older age group”.110
Research has also found that older people may face multiple kinds of family violence behaviours in combination. In particular, psychological abuse has been observed to accompany financial abuse, as it is thought that psychological abuse aids in grooming for and supporting ongoing financially abusive behaviours.111 An example is an adult child coercing their parent into believing they are no longer capable of controlling their own finances, and that this responsibility should be transferred to them.
Older people are unique from the general population of family violence victims in terms of demographic and relationship characteristics that are associated with victim-survivors and perpetrators. Victoria Police data provided to the RCFV showed that while older women were more likely than men to be affected parties in family violence incidents, “among people aged 65 and older, a higher proportion of victims are men than the proportion of male victims in the younger population”.112 This information indicates that while traditional roles of female victimisation are present in family violence involving older people, males appear more likely to be targeted in old age than at any other age bracket.
Evidence presented by the AIFS contends that most elder abuse perpetrated is intergenerational and typically involves sons perpetrating abuse against their mothers.113 This is consistent with research conducted by the National Ageing Research Institute, which analysed data derived from a record of calls to a helpline operated by Seniors Rights Victoria (SRV), and found that 67% of helpline calls concerned abuse committed by an adult child of the victim, while only 8% concerned abuse from a partner.114
The RCFV additionally noted that unrelated carers and co-residents in shared living facilities also perpetrate abuse against older people which can be considered family violence.115 The increased prevalence of older people who receive care in their home from carers, or who live in retirement villages or aged care facilities, means that this population is exposed to a wider range of potential perpetrators than other family violence victims. The extended definition of a family member discussed on page 29 explains how unrelated individuals may still be considered victims or perpetrators of family violence.
Under-reporting and barriers to accessing services
Under-reporting was recognised by the RCFV to play a major role in the absence of data surrounding older people and family violence.116 It is believed that most crimes against older people go unreported, largely because of complex dynamics and structures which discourage older people from reporting family violence.117
Additional reasons that older people may not disclose a family violence incident include:
- an expectation that women are to remain in abusive relationships, or that family violence matters should be dealt with privately or within the family118
- a failure to recognise that they are a victim of family violence, including a view that abusive behaviour is a normal part of relationships or of ageing119
- a reluctance to report an adult child in order to preserve family relationships or avoid invoking punitive actions against the perpetrator120
- a fear that if an abusive caregiver is removed, they will lose access to care, or will face an unchosen change in living circumstances121
Other issues contributing to the lack of data on family violence and older people include poor recognition from professionals working with older people of family violence and elder abuse indicators, a reluctance to report or respond to violence and abuse and a lack of infrastructure in place to collect adequate data on the subject.122
Why do we need to collect information on older people?
Presently, there is limited information collected in both surveys and administrative data which can be used to make informed decisions about service use, responsive intervention strategies and risk assessment factors. This section highlights current gaps in information concerning family violence and older people.
Gaps in information
Limited survey data
There are few large-scale national level surveys which directly inform about family violence and the experiences of older people. Population-based surveys which collect information about abuse of older people in Australia exist, however the scope and coverage of these surveys is limited. The Personal Safety Survey (PSS) developed by the ABS collects information from men and women aged 18 years and over about the nature and extent of experiences of violence since the age of 15 years.123 Although the survey does include responses from older people, the types of abuse included in the survey are limited to physical and sexual abuse, and to family violence within the context of intimate partner violence. The PSS therefore has limited information on types of family violence associated with elder abuse, including economic abuse or family violence that is committed by adult-children or other family members.
Another major national survey which includes information on abuse involving older people is the Australian Longitudinal Study of Women’s Health. This survey contains three cohorts of women of different ages, with one cohort comprised of women born between 1921 and 1926. The survey assesses women’s physical and mental health, as well as psychosocial aspects of health, including measures relevant to vulnerability, coercion, dependence and dejection.124 While this survey is better equipped to capture experiences of psychological abuse and neglect, a limitation is that it does not collect information on perpetrator type, nor does it collect information about the experiences of older males subject to family violence.
Limited scope of family violence services
Despite the broad definition of family violence used in the FVPA, this violence is still often understood as occurring primarily within the context of an intimate partner relationship, and being defined by physical or sexual violence. This is apparent within the scope of many surveys distributed concerning family violence, and in the range of support services offered in response to family violence incidents. In a statement to the RCFV, the Eastern Elder Abuse Network noted that “ the abuse of age specific services for older people experiencing elder abuse means that the abuse will continue to go unnoticed, unreported and unaddressed”.125 Further, the RCFV heard that there were few services for perpetrators of family violence against older people, with “most programs designed for men committing violence against their intimate partner”.126 The narrow scope of available services means that older people are often not included in data collected by family violence services.
Limited administrative data collected
In order to make informed decisions about family violence incidents and service use, high quality administrative data are needed. Gaps in administrative data concerning family violence and older people can be attributed to a number of issues including a reluctance by victims to report abuse, a lack of senior-specific services available to respond to family violence,127 cultural attitudes which normalise family violence behaviour against older people128 and a lack of knowledge by healthcare professionals to identify and respond to suspected family violence.129 Many of these issues combine to form a cycle which perpetuates the lack of data existing on older people and family violence.
Challenges in current data collection practices
Unlike other priority communities covered in this framework, older people can be easy to identify in data if an organisation collects information on a person’s age, and this information is often readily collected across services. Despite this, there are concerns about the under-representation of older people in data surrounding family violence. This may occur because identifying family violence may not be core to the business function of the mainstream organisations that provide services to older people, which can lead to a lack of direction from organisations to collect this type of information. The RCFV noted that aged care facilities and hospitals play “an important role in identifying, reporting and preventing elder abuse”.130 The RCFV heard that health care professionals are more likely to detect elder abuse if they routinely ask older people about abuse, if they have an elder abuse protocol and if they are trained on the relevant law regarding abuse.131 However many organisations that routinely interact with older people may not be collecting information on family violence, despite having opportunities to do so.
Data collection standards for collecting information on older people
Given that the defining characteristic of older people is their age, this framework does not introduce any elderly specific data items beyond those proposed in the ‘General data items’ section. Improvements to data collection practices should instead focus on collecting information which is core to the family violence conduct and that recognises that the type of incidents and perpetrators who are associated with this population may not fit into an organisation’s traditional definition of family violence. This includes:
- information about the type of family violence risk present, which may be any recognised evidence-based risk factor, such as emotional or economic abuse
- the relationship between parties, for example, sibling, child or familial-like carer
This will allow for higher level analysis of the collected information, and in time, grow the evidence base on the types of family violence experienced by this cohort. When collecting data from elderly people, practitioners should also be aware of intersectionalities that may impact a person’s capacity to provide accurate information. The disabilities section within this framework provides some advice on ways to collect data from people who require assistance to communicate, and those with a cognitive disability, which may be relevant to consider in relation to elderly people.
Training and resources
Elder abuse prevention and response online training
This free 2-hour online training course assists in building the capacity of the Victorian workforce to identify and respond to elder abuse.
Website: www.elderabuseprevention.e3learning.com.au
Integrated model of care for responding to suspected elder abuse
In response to the findings of the RCFV, the integrated model of care for responding to suspected elder abuse is being trialled at five health service locations to strengthen elder abuse responses and support across the care continuum. The integrated model of care is based on a least restrictive, clientcentred and family-inclusive framework.
Website: https://www.health.vic.gov.au/wellbeing-and-participation/integrated-model-of-care-for-responding-to-suspected-elder-abuse
Justice Connect Seniors Law
A service which provides free legal services to older people of limited financial circumstances, and assists with legal issues including guardianship and administration, powers of attorney and living
arrangements.
Website: www.justiceconnect.org.au/our-programs/seniors-law
Phone: 03 8636 4400
Seniors Rights Victoria
A state-wide service that provides information and responses for older people experiencing abuse.
Services they offer include a helpline, specialist legal services, community education and short-term support and advocacy for individuals.
Website: www.seniorsrights.org.au
Phone: 1300 368 821
95 Joosten, M, Dow, B & Blakely, J 2015, Profile of elder abuse in Victoria: Analysis of data about people seeking help from Seniors Rights Victoria, National Ageing Research Institute & Seniors Rights Victoria, Melbourne.
96 AIHW 2017, Older people, viewed 15 June 2018, https://www.aihw.gov.au/reports-statistics/population-groups/older-people/about
97 Ibid.
98 RCFV 2016, Volume 5 Report and recommendations, p.68.
99 Ibid p.69.
100 Kaspiew, R, Carson, R & Rhoades, H 2016, Elder abuse: Understanding issues, frameworks and responses, AIFS, Melbourne.
101 Ibid p.3.
102 Ibid p.11.
103 RCFV 2016, Volume 5 Report and recommendations, p.84.
104 Ibid.
105 Kaspiew, R, Carson, R & Rhoades, H 2016, Elder abuse: Understanding issues, frameworks and responses, AIFS, Melbourne, p.13.
106 RCFV 2016, Volume 5 Report and recommendations, p.86.
107 Kaspiew, R, Carson, R & Rhoades, H 2016, Elder abuse: Understanding issues, frameworks and responses, AIFS, Melbourne, p.11.
108 RCFV 2016, Volume 5 Report and recommendations, p.71.
109 Ibid p.69.
110 Kaspiew, R, Carson, R & Rhoades, H 2016, Elder abuse: Understanding issues, frameworks and responses, AIFS, Melbourne, p.7.
111 Ibid p.12.
112 RCFV 2016, Volume 5 Report and recommendations, p.69.
113 Kaspiew, R, Carson, R & Rhoades, H 2016, Elder abuse: Understanding issues, frameworks and responses, AIFS, Melbourne.
114 Joosten, M, Dow, B & Blakely, J 2015, Profile of elder abuse in Victoria: Analysis of data about people seeking help from Seniors Rights Victoria, National Ageing Research Institute & Seniors Rights Victoria, Melbourne.
115 RCFV 2016, Volume 5 Report and recommendations, p.71.
116 Ibid p.80.
117 Ibid p.11.
118 Ibid p.80.
119 Ibid.
120 Ibid.
121 Kaspiew, R, Carson, R & Rhoades, H 2016, Elder abuse: Understanding issues, frameworks and responses, AIFS, Melbourne, p.13.
122 RCFV 2016, Volume 5 Report and recommendations, p.81-82.
123 ABS 2017, 4906.0 Personal Safety, Australia, 2016, viewed 19 June 2018, https://www.abs.gov.au/AUSSTATS/abs@.nsf/Lookup/4906.0Explanatory%20Notes12016?OpenDocument
124 Australian Longitudinal Study on Women’s Health 2018, Study Overview, viewed 19 June 2018, https://www.alswh.org.au
125 RCFV 2016, Volume 5 Report and recommendations, p.88.
126 Ibid p.89.
127 Ibid p.88.
128 Ibid p.76.
129 Ibid p.77.
130 Ibid p.82.
131 Ibid.
Data collection standards - Lesbian, gay, bisexual, transgender and intersex communities
Highlights the family violence issues faced by LGBTI communities, existing data standards and guidelines used to collect information, and the challenges in collecting this data.
The RCFV noted that lesbian, gay, bisexual, transgender and intersex (LGBTI) people experience unique forms of family violence, and highlighted the lack of information, data and education that currently exists in this area.132 This section highlights the family violence issues faced by LGBTI communities, existing data standards and guidelines used to collect information, and the challenges in collecting this data. A data collection standard is presented which is recommended to be used for the collection of information about LGBTI people by agencies and service providers who respond to family violence or offer family violence services.
Terminology and definitions
Although lesbian, gay, bisexual, transgender and intersex communities are often grouped together because of a shared history of discrimination, each of these communities and the barriers they face are distinct.133 There are many people that make up these diverse groups, which extend beyond the five letters of ‘LGBTI’. However, this framework refers collectively to ‘LGBTI communities’, as this is the term used by the RCFV.
LGBTI communities describe themselves through the identification of their gender, sex, sexual orientation and intersex variation in a variety of ways. Definitions used in this section for gender identity, sex, sexual orientation and intersex can be found in both the ‘Data collection standard for collecting information about LGBTI people’ and the ‘Glossary’. The diagram below provides a basic overview of each concept and shows that while gender, sex and sexual orientation are connected to each other, they are also distinct. Additionally, there is more than one definition that exists for these concepts and associated terminology.
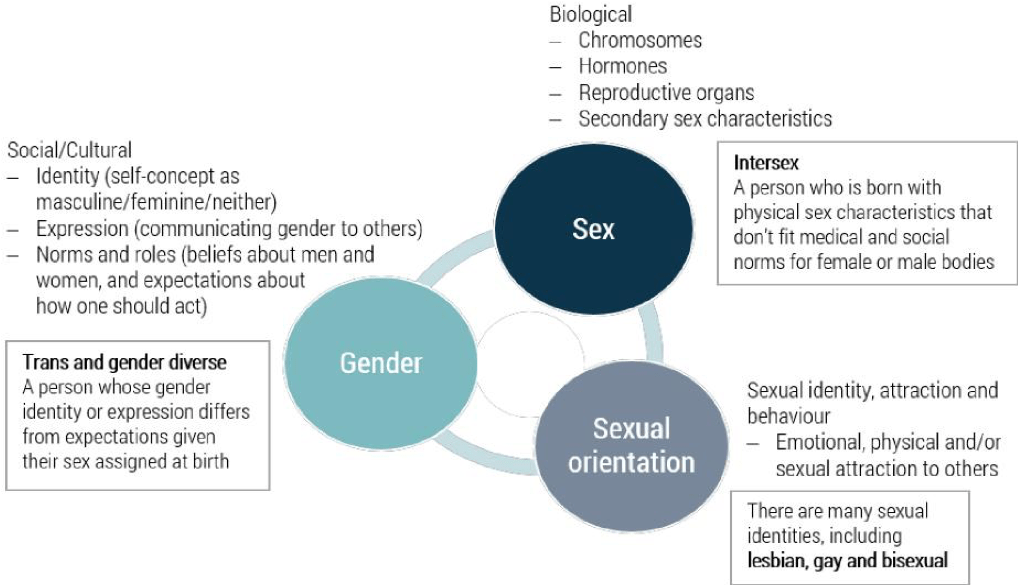
www.slideshare.net/jayembee/introduction-to-gender-minorities134
Family violence in LGBTI communities
Volume five of the RCFV report provides detailed information regarding what is known about the experience of family violence in LGBTI communities, and recommendations to address these issues. Summarised below are key points regarding prevalence, some of the unique forms of family violence in these communities and barriers to LGBTI services.
Prevalence
Currently, little is known about the prevalence of family violence in LGBTI communities. Available Australian research indicates that intimate partner violence in LGBTI communities is as prevalent as it is in the general population,135 with transgender and intersex people experiencing a higher prevalence of intimate partner violence compared to lesbian, gay and bisexual people who are not transgender and not intersex. Transgender women in particular are at greater risk of hate crime and sexual assault.136 Research in Australia regarding family violence in LGBTI communities beyond intimate partner violence is minimal.
Contributing circumstances and specific presentations of family violence risk
While it is vital to acknowledge that family violence is overwhelmingly committed by men against women,137 this focus has contributed to the lack of awareness of family violence experienced by LGBTI people. Assumptions can be made regarding family violence incidents which contribute to this. For example, an incident involving two men living together may not be recognised as family violence by police, and when viewed through the lens of heterosexual intimate partner violence, an assumption made that they are housemates. This could also be a contributing factor to some LGBTI people not recognising that what is happening to them constitutes family violence, which in turn may decrease the number of LGBTI people reflected in family violence data. Heteronormativity and heterosexism can also manifest in LGBTI relationships and this can contribute to the gendered drivers or presentations of risk in these communities.
In addition to the types of family violence which exist in the general community, there are specific ways that family violence may be present or experienced by LGBTI people. These include the following examples:
- emotional abuse:
- threatening to disclose someone’s gender identity, sex, sexual orientation or intersex variation (that is, outing someone) as a form of control
- telling a partner they will lose custody of their children as a result of being outed
- transphobic abuse whereby a person deliberately misgenders their transgender partner, ridicules their body or gender identity, or stops them from taking hormones or accessing services138
- a perpetrator claiming that the police, justice system or other support services are homophobic, biphobic or transphobic and won’t help the victim
- telling a person they deserve violence because they are lesbian, gay, bisexual, transgender or intersex
- telling a partner that the abusive behaviour is normal for a gay relationship, and that the abuse is mutual or consensual139
- sexual abuse, such as coercing sex through manipulation of the victim’s shame related to their sexual or gender identity
- physical violence committed by a family member due to their homophobia or transphobia
Under-reporting and barriers to accessing services
A small number of LGBTI-specific family violence support services and referral pathways exist, but there is currently a lack of services working with female perpetrators. Thorne Harbour Health (previously the Victorian AIDS Council) run the only Men’s Behaviour Change Program (ReVisioning) for gay or bisexual men in Victoria. Such services are often working over capacity with limited funding, and may be scarce or non-existent in rural, regional and remote areas.140
Trans and gender diverse people face particular barriers in escaping family violence and accessing housing support services. This is partly based on a lack of services designed to assist these communities.141
In addition, if service providers and agencies do not recognise the unique experiences of people in LGBTI communities, family violence may go unidentified and services may be inaccessible or inappropriate for both victims and perpetrators of family violence.
Why do we need to collect information about LGBTI people?
There is a lack of information, data and education both within LGBTI communities and in the broader community regarding family violence experienced by LGBTI people. The collection of information about LGBTI people can assist in addressing the gaps in data, and service response, which currently exist. Additionally, it was noted in consultation that many people feel supported and seen when their identity is represented in demographic data collection processes. It is acknowledged that questions regarding gender identity, sex, sexual orientation and intersex variation are personal, and may be seen by some as intrusive. With increased awareness and training, organisations will be better equipped to collect this information in an appropriate and inclusive way. Summarised below are key issues that were noted either in the RCFV findings or were found through research and consultation in regards to the increased demand for information about LGBTI people, and current gaps in information.
Increased demand for information about LGBTI people
Several submissions to the RCFV noted the importance of improved data collection in regards to LGBTI communities. The submission from Gay and Lesbian Health Victoria (GLHV) stated that enhanced data collection processes within the family services sector (utilising appropriate and sensitive approaches) would assist in the provision of important information for ongoing service development.142 The joint submission to RCFV from Safe Steps Family Violence Response Centre and No to Violence (NTV) recommended that:143
- the Victorian Government:
- supports agencies and government departments to review and update data collection capabilities to enable comprehensive information to be gathered on LGBTI communities
- supports and resources the creation of a state-wide data collection strategy for both family violence agencies and LGBTI organisations, which includes amending current data collection systems to ensure that consistent disaggregated data on LGBTI can be collected appropriately
- consultation needs to occur with LGBTI communities by agencies and policy makers as to howto ethically and respectfully collect relevant data.
Gaps in information
In recent years, following social and legislative reforms, LGBTI Australians have begun to be explicitly included in various public policies, programs and initiatives. However, many existing administrative data sets do not include categories to record if a person is LGBTI. This contributes to a significant information gap on the experiences of LGBTI people, and on their use of services. Further, family violence within LGBTI communities can also be under-reported due to narrower definitions that focus on intimate partner violence. It was noted in consultations for example that family members may commit violence against a child or sibling when they ‘come out’. There is currently limited data on the prevalence of this type of family violence.
More broadly, relationship type data are collected by some agencies and surveys such as the ABS Personal Safety Survey (PSS) and Crime Victimisation Survey (CVS), and when used in combination with a person’s sex or gender has been used to infer the number of same-sex relationships experiencing family violence (for example, a female victim in an intimate partner relationship with a female perpetrator). However this doesn't adequately capture the range of LGBTI people or relationship types. For example, victims who are bisexual but in a heterosexual relationship, relationships involving transgender or intersex victims, and victims experiencing family violence outside of an intimate partner relationship. It also relies on those collecting data to identify the relationship accurately, without making assumptions, and on data analysis and reporting systems that can facilitate more complex reporting and analysis.
Due to the lack of comprehensive data about LGBTI people, policy decision-makers must turn to LGBTI-targeted studies for evidence. Such studies are highly valuable but are unable to represent all LGBTI people, as coverage of the populations of interest is often limited, and not all LGBTI people are engaged with LGBTI communities.144
Challenges in current data collection practices
Regardless of an organisation’s willingness to collect information about gender, sex, sexual orientation and intersex variation, there are specific challenges that exist regarding data collection from LGBTI communities that organisations need to be aware of and consider. It is important to note that these challenges should not deter an agency from collection; rather, they should inform the organisation in their preparation for data collection. Challenges that are specific to a particular data item are explored under ‘Data collection standard for collecting information about LGBTI people’ on page 56. The challenges listed below are in addition to those discussed on pages 12 to 18, which are relevant to all priority communities within this framework.
Lack of knowledge about LGBTI communities
In order to collect high quality data, agencies need to be aware of and understand the needs of diverse LGBTI communities so that they may collect information appropriately, and provide an appropriate response. The joint submission to the RCFV from Safe Steps and NTV revealed that awareness of distinct LGBTI communities was variable among non-LGBTI specific service providers resulting in a lack of clarity around how to respond to subgroups and their specific needs.145 Additionally, it was noted in consultations that service providers and agencies may have unconscious bias, and make assumptions about a person’s gender identity or sexual orientation. If organisations lack knowledge about LGBTI communities, they may not feel comfortable asking about gender identity, sex, sexual orientation or intersex variation. Further, LGBTI people are not seen by all as groups as particularly vulnerable, despite extensive evidence regarding the stigma and discrimination they have experienced.146
Reluctance to disclose
Throughout consultation, it was acknowledged that some people will not be willing to disclose their gender identity, sexual orientation, sex or intersex variation. While attitudes are gradually changing, discrimination towards LGBTI people is still prevalent.147 Many do not trust police and the justice system, due in part to a history of discrimination, and the perception that they will not be taken seriously or believed. People may fear that an agency or service will be homophobic, transphobic or biphobic, or that the service won’t know how or be able to help them. In order to feel safe, they may have to hide their gender identity or sexuality, and by seeking help they may fear that this will further fuel discrimination against them. Additionally, unlike most other demographic information collected, the identity of a person who is LGBTI may not be known by people around them.148 There may also be a fear of disclosing to someone they already know in the community. As a result, some may fear the impact of revealing this information, so it is understandable that they may not feel comfortable or safe disclosing.
A person may give a different response to questions regarding gender identity, sexual orientation, sex or intersex variation, depending on the context of the situation. For example, the reason why the data are being collected, who will see the data, and the social or cultural setting.
Existing data standards
There is very little that exists in Australia in regards to data standards for collecting statistical information from LGBTI communities, despite social and legislative changes that have occurred in recent years. In 2013, the Sex Discrimination Act 1984 (Cth) was amended to introduce new protections from both direct and indirect discrimination on the grounds of sexual orientation, gender identity and intersex status in many areas of public life.
Sex and gender
The legal protections provided by the change to the Sex Discrimination Act 1984 (Cth) are complemented by the Australian Government Guidelines on the Recognition of Sex and Gender. These guidelines recognise that an individual may identify as a gender other than the sex they were assigned at birth, or may not identify exclusively as male or female, and that this should be reflected in records held by the government.149
| Australian Government Guidelines on the Recognition of Sex and Gender (the Guidelines) |
|---|
|
The Guidelines:
The Guidelines commenced on 1 July 2013, and state that all Australian Government departments and agencies are expected to progressively align their existing and future business practices with these Guidelines by 1 July 2016. The Guidelines’ preferred approach is for Australian Government departments and agencies to collect gender information rather than sex. They acknowledge that people may identify as a gender other than the sex they were assigned at birth, and that people may not identify as exclusively male or female. The Guidelines propose that a third category for gender and sex is to be collected and recorded as X (indeterminate/intersex/unspecified).150 |
The ABS released the Standard for Sex and Gender Variables (the ABS Standard) in 2016. It was developed with consideration to the Guidelines, and replaced the Standard for Sex Variable 1999. The introduction of the ABS Standard is a move towards being able to collect data from trans and gender diverse communities, as it includes information regarding the distinct concepts of gender and sex, and its classification is no longer binary (ie. ‘female’ and ‘male’ only). The ABS Standard introduced a third category for both sex and gender of ‘other’, with the 2016 Census being the first in Australia to include this third category (when a special form was requested). The ABS Standard follows the Guidelines’ approach regarding the collection of gender rather than sex, and states that sex should only be collected when there is a legitimate need to collect it.
There are limitations to the Guidelines and the ABS Standard in their current forms. The ABS Standard states that further breakdown of the third ‘other’ category is recommended only when undertaking an in-depth social study.151 This may promote the idea that people who do not identify as female or male do not always need to be included in data. 152 Without consistent inclusion (where possible and appropriate), it is not possible to create an evidence base for these populations. Additionally, the ‘other’ category has been considered stigmatising,153 and amongst groups consulted in the development of this framework, this term was not favoured. The ABS Standard uses terminology recommended by the Guidelines, in that “terms such as ‘indeterminate’ and ‘intersex’ are variously used to describe the third category of sex”.154 The Sex and Gender Advisory Group155 have stated that the use of the term indeterminate implies a lack of a determined category. The group notes that people who do not identify as women or men in terms of gender and, separately, people whose bodily characteristics are not considered stereotypically female or male, are not ‘indeterminate’ and often have clearly determined ways of categorising themselves.156 Additionally, the group considers the use of X to represent intersex as inappropriate and inaccurate in capturing data from intersex people.157 The National LGBTI Health Alliance’s White Paper also noted that most people who are intersex do not wish to be considered as a third sex, and many identify their sex as female or male.158 These current limitations show that the ABS Standard in its current form may not be effective in accurately capturing data from these diverse populations.
Research has been undertaken on, and some changes made to, gender standards internationally. In 2015, Statistics New Zealand introduced the Statistical Standard for Gender Identity. This standard classification has three response categories; ‘male’, ‘female’ and ‘gender diverse’, and recommends that ‘gender diverse’ has a write-in facility to allow respondents to fully describe their gender identity. ‘Gender diverse’ has a further level of classification for outputs which has four categories.159 The Office for National Statistics (ONS) in the United Kingdom, in collaboration with the Equality and Human Rights Commission (EHRC), have undertaken research into the collection of gender identity. Whilst the focus of their research has largely related to the inclusion of questions in the Census, it also looked at other options for meeting data requirements, starting with the exploration of administrative data.160
Sexual orientation
There is no ABS standard that currently exists in Australia for the collection of sexual orientation data. The ABS General Social Survey (GSS) included a question regarding sexual orientation for the first time in 2014, and over half a million people (approximately 3% of the Australian adult population) identified as gay, lesbian, bisexual or another sexual orientation which was not heterosexual. Whilst the GSS does not ask questions regarding family violence, results indicated increased vulnerability in related areas for those who did not identify as heterosexual, such as discrimination, homelessness and mental health conditions.161
A single standardised measure of sexual orientation is contained in most Statistics Canada data sets, and in the United States, multiple measures of sexual orientation are often present in data sets from the National Center for Health Statistics.162 In the United Kingdom, the National Health Service (NHS) has created an information standard for collecting sexual orientation data, in collaboration with the LGBT Foundation. The standard “provides the mechanism for recording the sexual orientation of all patients/service users aged 16 years and over across all health services with responsibilities for adult social care in England where it may be relevant to record this information”.163 The question set is based on research on sexual identity conducted by the ONS and EHRC, and on current practice by organisations which collect sexual orientation information. Their proposed question has the following seven response options; heterosexual or straight, gay or lesbian, bisexual, other sexual orientation not listed, person asked and does not know or is not sure, not stated (person asked but declined to provide a response) and not known (not recorded).164
Data collection standard for collecting information about LGBTI people
The data items included in this data collection standard are based on what is currently recommended in practice and research, and the findings of our consultations with organisations in Victoria.
There are some privacy implications related to the collection of data items in this standard due to their sensitive nature, and relevant privacy legislation including the Health Records Act 2001 (Vic) and the Privacy and Data Protection Act 2014 (Vic) should be considered by data custodians when collecting and storing this information. Further information about privacy and security considerations is provided on page 18.
All data items in this data collection standard should only be used in the appropriate service context. For example, it may be inappropriate to ask about someone’s sexual orientation during the first interaction with a person in a crisis situation. Before using a data item in this standard, the information that will be gained from it needs to be considered. The purpose of collecting data needs to be made clear to the client, and should be able to be linked to either a direct service response or referral to an appropriate service. The communities that make up ‘LGBTI’ are diverse, and it is not possible to capture information from these populations in a single data item. However, it may not be appropriate to use all four data items. While this data collection standard aims to inform organisations of the most appropriate data items to use to collect data from LGBTI communities, it is not intended as a guide for when to collect this data.
It has been previously noted that organisational change and staff training relating to LGBTI inclusive practice is vital, but its importance is emphasised again here. It is important to avoid making assumptions about a person’s gender identity, sex, sexual orientation or intersex variation. Without educating staff, there is a risk of misgendering165 or incorrectly interpreting a family violence situation, and causing harm to clients. Staff need to be trained in recognising when it may not be appropriate to ask, and in how to sensitively and respectfully collect data. For information regarding some organisations which offer LGBTI inclusive training in Victoria, please refer to ‘Training and resources’.
Although mentioned previously in the framework, it is worth noting again the importance of confidentiality, and how this specifically relates to LGBTI communities. As stated in the Rainbow Tick guide to LGBTI-inclusive practice, “disclosure has the potential to significantly impact on an LGBTI person’s safety, health and wellbeing and their social connectedness...this may create real tensions for the LGBTI consumer regarding confidentiality and unintended disclosure”.166 If someone does not wish to disclose information, that is their choice and it should be respected.
While this data collection standard is a step forward in collecting information from LGBTI communities, definitions used throughout the standard are based on current language and terminology, and it is important to keep in mind that these definitions will continue to change and evolve. Therefore, the terms used in the standard should be reviewed and updated over time to ensure they remain applicable and relevant.
This data collection standard provides information regarding inclusive language, and covers the following four data items:
- gender identity
- sex
- sexual orientation
- intersex
Although this data collection standard follows the approach of the Guidelines and the ABS Standard of collecting gender identity in preference to sex, information regarding sex has been included for several reasons, including the potential for improved data collection from transgender populations when combined with a gender identity question (also known as the two-step approach). Further information regarding the two-step approach is included under the gender identity and sex data items.
Using Inclusive language
The language that is used when talking to someone about their gender identity, sex, sexual orientation or intersex variation needs to be appropriate, sensitive and inclusive. Using inclusive language decreases the risk of misgendering a client, minimises harm, shows respect and has the ability to help build positive relationships with clients. From a data collection point of view, it is likely that the use of inclusive language increases the accuracy of the data collected.
Just as assumptions should be avoided regarding a person’s gender identity, sex, sexual orientation or intersex variation, it is important to avoid making assumptions about how someone wishes to be addressed and describes themselves. Whenever possible, questions should be asked privately to minimise discomfort or harm to a client.167
Names, pronouns and titles
A person’s name on identification documents, such as their driver’s license, may not match the name that they use. When a person discloses that they have a name that they use other than the name on their identification documents, an agency or service should ensure that they use this name when communicating with this person. Both the name that a person uses, and name/s on their official documentation, should be collected. See the ‘General data items’ section for information regarding the collection of name data.
Pronouns can imply someone’s gender, for example, describing someone as ‘he’ or ‘she’. People with non-binary genders often prefer pronouns that aren’t gendered, such as ‘they’. Some people prefer to be described with their first name only or may prefer no pronoun at all.168
Intersex people and transgender people who identify as women or men can feel excluded when
people avoid pronouns or use gender neutral language. Using inclusive language means referring to an intersex or transgender woman who identifies as a woman as ‘her’, ‘she’, or, ‘the woman’.169
Forms requiring a person to select a title should include ‘Mx’ as an option, which is used by some people with non-binary genders. Where possible, the inclusion of a free text option so that someone can self-describe is recommended. It is also important to know that some people do not use a title.
Inappropriate or offensive terms and language
The use of inappropriate language can make it difficult for LGBTI people to engage with services and can cause harm to LGBTI clients. If a person accidentally misgenders a client, or uses inappropriate language, apologise briefly and start using inclusive language.170 The below lists some examples of language and terms which should be avoided.
- Although intersex people may use a variety of terms to describe themselves, it is considered insensitive for others to describe intersex people as ‘hermaphrodites’ or as having ‘disorders of sex development’.171
- It is considered insensitive to assume that someone identifies as trans based on their history, or, to call some ‘a trans’ or ‘a transgender’.172
- Do not call an intersex woman or transgender woman ‘he’, ‘it’, ‘the person’, or avoid pronouns.
- Do not use the terms ‘preference’, ‘preferred’ and ‘lifestyle’ in relation to a person’s gender identity or sexual orientation. These terms suggest that a person’s identity is chosen, rather than who they are.
- Avoid language which assumes all relationships are heterosexual. It is better to use the word ‘partner’ than ‘wife/husband’ when the gender, sexual orientation or relationship status of a person is unknown. When someone mentions their children, do not make the assumption that the person is in a heterosexual relationship.173
For more information regarding inclusive language, see:
- Making your service intersex friendly, a guide created by Intersex Human Rights Australia, available on their website www.ihra.org.au/services
- Inclusive language guide: respecting people of intersex, trans and gender diverse experience, available on the National LGBTI Health Alliance website www.lgbtihealth.org.au
- Victorian Public Sector inclusive language guide, available at www.vic.gov.au/equality
- Policy and practice recommendations for alcohol and other drugs service providers supporting the trans and gender diverse community, available at www.vac.org.au
For information regarding some organisations which offer LGBTI inclusive training in Victoria, please refer to ‘Training and resources’.
Gender identity
In line with the Australian Government Guidelines on the Recognition of Sex and Gender (the Guidelines) and the ABS Standard, this data collection standard recommends collecting gender identity in preference to sex.
Definition
Gender refers to the socially constructed categories assigned on the basis of a person’s sex. While other genders are recognised in some cultures, in Western society, people are generally expected to conform to one of two gender roles matching their sex; male = man/masculine, and female = woman/feminine. Gender norms define how a person should dress and behave, and the roles people have in society.174 Gender identity refers to a person’s internal and individual sense of gender which is not always exclusively masculine or feminine, and may or may not correspond to their sex.175
Affirming one’s gender is a deeply personal decision that involves a person seeking to redress a mismatch between their assigned sex at birth and their gender identity. It does not necessarily involve surgery; it means that a person is living their affirmed gender.176
Question phrasing and response categories
|
What gender do you identify as? □ Male |
Standard answer categories
Gender diverse is an umbrella term which encompasses gender identities and expressions that are different from a person’s sex assigned at birth,177 and can include people who identify as transgender, agender (having no gender), bi-gender (both a woman and a man) or non-binary (neither woman nor man).178 Transgender (or trans) is a term used by some people who experience or identify their gender as not matching their sex assigned at birth.179 However, it is important to remember that not all gender diverse people are transgender,180 and many people of transgender experience live and identify as women or men, and may not have a ‘trans gender identity’.181 There is no one ‘correct’ or ‘complete’ way for trans and gender diverse people to express themselves.182
Aboriginal and Torres Strait Islander people may use the terms Brotherboy and Sistergirl in a number of different contexts, however, they are used in some Aboriginal communities to refer to trans and gender diverse people.183 Sistergirls are Aboriginal and Torres Strait Islander women who were classified male at birth but live their lives as women, including taking on traditional cultural female practices. Brotherboys are Aboriginal and Torres Strait Islander men who were classified female at birth but live their lives as male.184 These communities may not identify with western transgender terminology,185 and western terms (for example, ‘Aboriginal transgender woman’) may be seen as insufficient due to the complex connection to culture that shapes these communities.186 When a Brotherboy or Sistergirl client answers a question about gender identity verbally, the data collector should ask which response category they feel best describes them, rather than making assumptions.
To collect data on gender diverse people, this framework uses the inclusive term of ‘self-described’ rather than ‘other’. As language used to describe gender identities is evolving, having broader terms will decrease the risk of this data item becoming outdated and no longer relevant. The inclusion of a ‘please specify’ free text option within the ‘self-described’ response option allows a person to selfidentify. It is acknowledged that some systems may not be able to practically accommodate free text, either due to software restrictions, or the lack of resourcing associated with coding free text. However, having this capability means that people may be more willing to respond, and, where possible and appropriate, would enable more detailed information which is useful for the refinement of data collection and understanding of clients. As some people may not be willing to self-disclose, the inclusion of a ‘prefer not to say’ response category is recommended.
It is acknowledged that ‘male’ and ‘female’ are terms used to describe biological sex rather than gender. However, these are the terms used in national standards. When standards (such as the ABS Standard) are revised, and if language used in such standards change, it will be necessary to review these response options. Research from the EHRC in the UK found that “despite concerns raised in focus groups around the potential confusion of using traditional sex categories when asking how one describes themselves (i.e. about gender), evidence from cognitive interviews suggests that the categories ‘male’ and ‘female’ do work, and they work well for both trans and non-trans individuals”.187
Sex
Although the framework follows the recommendation of the Guidelines and the ABS Standard regarding the collection of gender identity in preference to sex, information regarding sex has been included in the framework. Sex is still considered by many as a primary means of measuring and analysing many aspects of the population, and continues to be collected in the Census. It is also a key variable used in Statistical Linkage Keys (SLKs), which are relied on to identify unique individuals accessing services and link data between agencies and service providers.
It is important to note that it is not recommended that all agencies collect sex information. Sex should only be asked if there is an operational requirement for the agency. As previously noted, the purpose of collecting either sex or gender identity, or both, must be considered prior to collection.
Definition
Sex refers to the biological characteristics of a person, which include chromosomes, hormones and reproductive organs. Sex assigned at birth refers to the sex category assigned to a person when they were born. Although sex and gender are conceptually distinct, these terms are commonly used interchangeably, including in legislation.188
Question phrasing and response categories
|
What sex were you assigned at birth (i.e. what was specified on your original birth certificate)? □ Male |
Standard answer categories
In Victoria, currently only one sex (M or F) can be registered at birth. Changes may be made in the future to include another option at birth, and if this occurs in Victoria, this data item may need to be revised and an additional response category added.
Although there are current data collections that include response categories such as ‘indeterminate’, this is generally only a code that is used for infants aged less than 90 days. As previously noted, the Sex and Gender Advisory Group189 have stated that people whose bodily characteristics are not considered stereotypically female or male are not ‘indeterminate’ and often have clearly determined ways of categorising themselves.190
As previously noted in ‘Existing data standards’, most people with an intersex variation do not consider themselves to be a third sex. Thus, the inclusion of an ‘intersex’ response category is unlikely to accurately capture intersex populations, and a separate question is recommended to collect information from people with an intersex variation (see the ‘intersex’ data item on page 63 for more information).
As some people may not be willing to self-disclose, the inclusion of a ‘prefer not to say’ response category is recommended.
Trans-gender
There are many people of transgender experience who live and identify as women or men and may not have a ‘trans gender identity’. The two step approach, described below, has been identified as one means of enabling more trans and gender diverse people to be included in data sets. In addition, some DHHS data sets have included a transgender data item that more directly allows a person to identify themselves as transgender. As some people may not be willing to self-disclose, the inclusion of a ‘prefer not to say’ response category is recommended.
|
Do you identify as transgender? □ Yes |
| Two step approach to collecting sex and gender identity |
|---|
|
Most current research notes that the two step approach enables more trans and gender diverse people to be included in data.191, 192, 193, 194, 195, 196, 197 The two step approach is when a question regarding gender identity is used in conjunction with a question regarding sex. For example, if someone responds to a question regarding gender identity with ‘male’ and responds to a question regarding sex assigned at birth with ‘female’, this information might be used together to infer that this person should be included in the transgender population. Research undertaken regarding this approach has mostly been in the context of data collection via surveys, or health organisations collecting data in situations where asking sex has been operationally required. Thus, it is unclear if the two step approach is appropriate for the collection of administrative data in a family violence context. Additionally, asking a transgender person’s sex assigned at birth may trigger negative feelings. With the added vulnerability of a family violence situation, there may be risk in asking about a transgender person’s sex due to safety concerns. |
Considerations in asking gender identity, sex and transgender identity
Asking someone a question about their gender identity allows for responses that are not necessarily binary (female/male).198 People are more likely to respond affirmatively to questions that use language with which they are comfortable, and less likely to respond accurately to questions that misgender them.199
Gender identity can change over time, as can a person’s willingness to self-disclose. Information should continue to be collected, when appropriate, even if a person comes into repeat contact with a service, and it is recommended that there is the capability to change these fields in the data.
As previously mentioned, the purpose of collecting information from each data item in this framework needs to be made clear to the client, and information gained should be used to inform either a direct service response or referral to an appropriate service. Relevant privacy principles should always be considered when making the decision to collect sensitive information.
Sexual orientation
Definition
Sexual orientation encompasses several dimensions of sexuality including sexual identity, attraction and behavior,200 and refers to a person’s emotional, physical and/or sexual attraction to another person.201 The data being collected in this data item is most closely related to sexual identity, which is the self-identified label that a person may choose to describe themselves.202 As sexual identity is just one aspect of sexual orientation, this data item will not capture other aspects of sexual orientation (i.e. attraction and behaviour). For example, a man that identifies as straight but has sex with men.
Sexual orientation has been chosen as the term in this framework as it follows the work that has been done internationally in this space203 that most closely reflects the purpose of this framework. It is also a more familiar term to the broader community. It may be appropriate in the future to change terminology if questions on other aspects of sexuality become more widely understood.
Question phrasing and response categories
|
How would you describe your sexual orientation? □ Straight or heterosexual |
Standard answer categories
Definitions for the terms used as response categories are as follows:
- Straight/Heterosexual – a person who experiences attraction (romantic, sexual, affectional, and/or emotional) solely or primarily to people of the opposite sex and/or gender.
- Gay/Homosexual – a person who experiences attraction (romantic, sexual, affectional, and/or emotional) solely or primarily to people of the same sex and/or gender. Although it may be used by people of all sexes and/or genders, it is more commonly used by men.204
- Lesbian – a woman who experiences attraction (romantic, sexual, affectional, and/or emotional) solely or primarily to other women.205
- Bisexual or Pansexual – a person who experiences attraction (romantic, sexual, affectional, and/or emotional) to more than one gender.206 People who are pansexual may seek to express that gender does not factor into their own sexuality, or, that they are attracted to trans and gender diverse people who may or may not fit into the binary gender categories of male and female. This does not mean, however, that people who identify as bisexual are focused on traditional notions of gender.207
- Asexual – people who do not experience sexual attraction, although this does not preclude romantic attraction.
Note that gay, homosexual and lesbian have been grouped as the aim of this data item is to identify sexual orientation rather than gender. Although bisexual and pansexual are different sexual identities, they have been grouped due to the overlap that exists in their meaning.
As with the gender identity data item, the inclusion of a ‘please describe’ free text option is recommended, however it is acknowledged that some systems may not be able to accommodate free text, either due to software restrictions or the lack of resourcing associated with coding free text.
This data item includes a ‘don’t know’ option and, as some people may not be willing to self-disclose, the inclusion of a ‘prefer not to say’ response category is also recommended.
Considerations in asking sexual orientation
Unlike gender or sex, sexual orientation is not a question that is routinely asked of people in Australia. Research done by the LGBT Foundation in England indicated that 90-95% of people would be comfortable disclosing their sexual orientation as part of demographic data collection if they understood why it was being collected.208 In preparation for their 2021 Census, the ONS in the United Kingdom tested the inclusion of a sexual identity question and evidence suggests the question is broadly acceptable and will not have a significant impact on overall response. Although the context of a census is different to the context of this framework, it is worth noting these findings.
NHS England, in collaboration with the LGBT Foundation, created their question set for sexual orientation based on research conducted by the ONS and the EHRC, and on current practice by organisations which collect data on sexual orientation. This has helped to inform the creation of the sexual orientation data item in this framework. Their standard covers all adults (i.e. those aged 16 and over) and although this standard is closely aligned with the NHS standard, it does not dictate the age at which this question should be asked by an organisation. As noted at the beginning of the data collection standard, organisational change and staff training is vital to ensure sexual orientation can be collected in the appropriate context, in an inclusive and sensitive way.
As the sexual orientation people identify with can change over time, as can a person’s willingness to self-disclose, information should continue to be collected even if a person comes into repeat contact with a service. Thus, there should be the capability to change this data field over time.
Intersex
Definition
Intersex people are born with sex characteristics that do not fit medical norms for female or male bodies.209 These characteristics can be physical, hormonal or genetic. Many forms of intersex exist, with more than 40 different variations known. Intersex variations may be apparent at birth or diagnosed prenatally. Some intersex traits become apparent at puberty, or when trying to conceive, or through random chance.210
Question phrasing and response categories
Intersex is a term for people born with atypical physical sex characteristics, and there are many different intersex traits or variations.
| Do you have an intersex variation? □ Yes □ No □ Prefer not to say |
Intersex people have a diversity of sex characteristics and gender identities. Most intersex people identify their sex as male or female, and do not wish to be considered a third sex.211 Thus, adding an ‘intersex’ category to a question regarding sex or gender identity is not appropriate, and a separate question is required to collect data from intersex populations. Separating intersex from a question on sex and/or gender avoids misgendering people with intersex variations and inadvertently including people who mistake intersex for a gender identity.212
It should not be assumed that respondents will understand what is meant by the term intersex, and it is recommended that the short descriptive statement preceding the question ‘Do you have an intersex variation?’ is used.
As some people may not be willing to self-disclose, the inclusion of a ‘prefer not to say’ response category is recommended. Additionally, it is recommended that only one response is accepted for this data item.
Training and resources
In order for organisations to be able to sensitively collect data from LGBTI people in the appropriate contexts, organisations need to ensure that their policies and procedures are inclusive of LGBTI people, and staff must be trained in practice which is LGBTI inclusive. The list of organisations below is not exhaustive, but seeks to provide some valuable resources for agencies and service providers in Victoria. Please note that many of the organisations listed are not-for-profit, with limited funding available for the services they provide. Thus, the training noted here may not be available on an ongoing basis. The information below is sourced from the websites of the organisations listed, and the National LGBTI Health Alliance’s professional development, education and training list, https://www.lgbtiqhealth.org.au/member_training_courses.
Training
Gay and Lesbian Health Victoria
GLHV offers a range of training options aimed at improving the quality of services organisations provide to LGBTI people. For more information, visit www.glhv.org.au/training or phone 03 9479 8760. Available training includes:
- Living LGBTI – a half-day training session which explores the ways in which discrimination affects the health and wellbeing of LGBTI people’s everyday lives.
- LGBTI diversity in aged care – a one day training session which promotes awareness of the range of issues facing older LGBTI people, provides information about relevant policy and legal issues, and focuses on inclusive care for LGBTI clients and residents.
- HOW2 Program – four workshops run over six months which promote the development of LGBTI-inclusive health and human services and assists organisations in the implementation of practices, protocols and procedures. The HOW2 program is based on a set of six ‘Rainbow Tick’ national standards for health and human services which were developed by GLHV in conjunction with Quality Innovation Performance (QIP). It is important to note that although the program is based on these standards, completion of the HOW2 program does not result in the awarding of a Rainbow Tick. In order for an organisation to obtain the Rainbow Tick, it must be formally accredited through an external process undertaken by QIP.
For more information, visit https://www.qip.com.au/standards/rainbow-tick-standards/.
Intersex Human Rights Australia (formerly known as OII Australia)
IHRA is a national not-for-profit organisation promoting human rights for intersex people, and provides information, education, and support. IHRA can offer custom training and education, which includes advice on the impact of legislation and regulations, human resources and equal opportunity issues. For further information, visit www.ihra.org.au/services.
Minus18
Based in Melbourne, Minus18 is Australia’s largest youth-led organisation for LGBTI youth. Minus18 offer 60-90 minute training sessions, with content which can be tailored to an organisation’s needs. For more information, visit www.minus18.org.au/index.php/workshops/adult-professional-training. Current available training includes:
- Sexuality and gender – explores issues affecting LGBTI youth, and equips attendees with tools to build LGBTI inclusivity into an organisation
- Supporting trans and gender diverse youth – provides an in-depth understanding of the issues trans and gender diverse youth face, with guidance to create supportive working solutions such as policy and procedure updates
Pride Inclusion Programs
Pride Inclusion Programs are social inclusion initiatives of ACON. Pride in Diversity is a national notfor- profit employer support program for LGBTI workplace inclusion specialising in HR, organisational change and workplace diversity, and Pride in Health and Wellbeing is a national membership program that provides year-round support in the provision of LGBTI inclusive services for those working within the health and wellbeing sector. For more information visit www.prideinclusionprograms.com.au and www.acontraining.org.au.
Transgender Victoria
Transgender Victoria (TGV) educates organisations and workplaces on how to provide better services for trans and gender diverse people, and seeks ways to provide direct services to these communities. For more information, visit www.transgendervictoria.com or phone 03 9020 4642. Current available training includes:
- LGBTI training – a 3 hour session which explores LGBTI inclusive practice, and differences between sexual orientation, gender identity and people with intersex characteristics.
- Trans and gender diverse introduction – a 2-3 hour session which covers areas of disadvantage and discrimination for trans and gender diverse people and related mental health impacts, legislative obligations, and provides suggestions/tips on working with trans and gender diverse people.
- LGBTI aged care sector training – a 3 hour session in LGBTI inclusive ageing and aged care training for all people involved in the aged care sector, providing attendees with more confidence to deliver inclusive, best practice service.
Thorne Harbour Health
Thorne Harbour Health (THH, previously known as the Victorian AIDS Council) advocate to improve health outcomes for sexually and gender diverse people, and have 35 years of experience working with these communities. THH run the only Men’s Behaviour Change Program for gay, bisexual, and queer men (including transgender men), and offer flexible support packages for LGBTI people experiencing family violence.
THH Education and Training aims to develop the workforce, improve sector capacity and increase awareness of the unique and complex vulnerabilities in LGBTI communities. THH training promotes a safe learning environment to enable useful discussions and interactions to take place between participants and facilitators. Education and training areas include:
- LGBTI cultural competency and sensitivity
- trans and gender diverse cultural competency and sensitivity
- family and intimate partner violence within LGBTI communities
- alcohol and drug use within LGBTI communities
- mental health and LGBTI communities
- sexual health and LGBTI communities
For more information, visit https://thorneharbour.org or phone 03 9865 6700.
Zoe Belle Gender Collective
The Zoe Belle Gender Collective are an online not-for-profit organisation which provides support, training and resources for Victorian trans and gender diverse communities. The youth project officer, Starlady, offers training which gives an introduction to trans and gender diverse youth inclusive practice which ranges between 1 and 3 hours. For further information, visit www.zbgc.com.au/transgender-gender-diverse-youth-training/ or phone 03 9448 6141.
Other resources
The below lists websites that contain a variety of information regarding LGBTI communities, and many offer valuable services to these communities and the wider population.
Please note that the organisations which offer training, listed above under ‘Training’, also have a vast amount of information available on their websites.
Anti-Violence Project Victoria
Victoria’s Anti-Violence Project are a not-for-profit organisation leading discussion on violence and its impacts on LGBT people and intersex people who identify with the sexually and gender diverse community. Anti-Violence Project provide an online portal for those wishing to report violence, and liaise with Victoria Police and other agencies to assist victims.
Website: www.antiviolence.info
Bisexual Alliance Victoria
Bisexual Alliance Victoria Inc. is a non-profit volunteer-run organisation dedicated to promoting the acceptance of bisexuals in LGBTI and mainstream society, providing a fun, safe space where bisexuals can meet, make friends, and talk about their experiences, and informing the bisexual community about relevant news and opportunities for activism.
Website: www.bi-alliance.org
Melbourne Bisexual Network
The Melbourne Bisexual Network aims to raise awareness around the unique health and wellbeing issues that face people who are multi-gender attracted, and to collectively determine strategies to improve and promote bi-inclusivity in LGBTQIA+ programs and services.
Website: www.melbournebisexualnetwork.com
National LGBTI Health Alliance
The National LGBTI Health Alliance is the national peak health organisation in Australia for organisations and individuals that provide health-related programs, services and research focused on LGBTI people. Much of the information produced by the National LGBTI Health Alliance has been referenced throughout this section, and is available on their website.
Website: www.lgbtihealth.org.au
The Fenway Institute – Do ask, do tell
A US-based toolkit for collecting data on sexual orientation and gender identity in clinical settings.
Website: www.doaskdotell.org
US National LGBTI Health Education Center
This website features useful webinars, including collecting data on sexual orientation and gender identity in the electronic health record: why and how.
Website: www.lgbtihealtheducation.org/training/on-demand-webinars
queerspace (located at Drummond Street Services)
queerspace is an LGBTI health and wellbeing support service with a focus on relationships, families, parenting and young people. queerspace services deliver counselling and case management for a range of issues, including intimate partner and family violence.
Website: www.queerspace.org.au/
Victorian Equal Opportunity and Human Rights Commission
The Victorian Equal Opportunity and Human Rights Commission (VEOHRC) is an independent statutory body with responsibilities under the Equal Opportunity Act 2010 (Vic), Racial and Religious Tolerance Act 2011 (Vic), and the Charter of Human Rights and Responsibilities, and they provide information pertinent to these three laws. VEOHRC also provide a free phone enquiry line and free dispute resolution services. Their website contains a variety of information, including guidelines for family violence services and accommodation, and for transgender people at work.
Website: www.humanrightscommission.vic.gov.au
Glossary
This glossary is based on the format of the LGBTIQ+ communities glossary created by the Australian Institute of Family Studies (AIFS) Child Family Community Australia,213 in that terminology is organised into the following categories:
- bodies and gender
- sexual orientation
- societal attitudes and issues
A range of sources have been used which contain further terminology and information, which include the LGBTIQ+ communities glossary noted above as well as the following:
- Inclusive language guide: Respecting people of intersex, trans and gender diverse experience (National LGBTI Health Alliance).214
- Addressing sexual orientation and sex and/or gender identity discrimination: Consultation Report (Australian Human Rights Commission).215
- LGBTI Data: Developing an evidence-informed environment for LGBTI health policy (National LGBTI Health Alliance).216
- Trans Pathways: the mental health experiences and care pathways of trans young people (Telethon Kids Institute Australia).217
- Guideline: Transgender people at work – Complying with the Equal Opportunity Act 2010 in Employment (VEOHRC).218
- From Blues to Rainbows: Mental health and wellbeing of gender diverse and transgender young people in Australia (ARCSHS, La Trobe University).219
- Making your service intersex friendly (IHRA and ACON).220
- LGBTI people and communities (LGBTI Health Alliance).221
- Transgender Victoria definitions.222
- Transcend support terminology and inclusive language.223
- Rainbow eQuality guide definitions (Department of Health and Human Services).224
- Bisexual Alliance Victoria Inc website.225
- Sexuality and gender terms (University of WA).226
- Intersex Human Rights Australia (IHRA) website.227
Definitions used are based on current language and terminology, and it is important to keep in mind that these definitions will continue to change and evolve. This glossary contains many key terms, but is not an exhaustive list of all terms that are used to describe gender, sex, sexual orientation and intersex.
Bodies and gender
Gender – refers to the socially constructed categories assigned on the basis of a person’s sex. While other genders are recognised in some cultures, in Western society, people are expected to conform to one of two gender roles matching their sex; male = man/masculine, and female = woman/feminine.
Gender binary – the classification of gender into two categories of man/woman.
Gender norms – relate to how a person should dress and behave, and the roles people have in society.
Gender identity – refers to a person’s internal and individual sense of gender which is not always exclusively masculine or feminine, and may or may not correspond to their sex.
Gender diverse – a term which encompasses all gender identities and expressions that are different from a person’s sex assigned at birth. Includes people who identify as agender (having no gender), as bi-gender (both a woman and a man) or as non-binary (neither woman nor man), and some nonbinary people identify as genderqueer or as having fluid genders.
Transgender or Trans – a person whose gender identity does not align with their sex assigned at birth. Trans is an umbrella term that includes a wide variety of identities. Not everyone who falls under this umbrella refers to themselves as ‘trans’. For example, while some women who have transitioned or affirmed their gender may refer to themselves as trans women, others may simply refer to themselves as women, and others will use a variety of terms. There is no one ‘correct’ or ‘complete’ way for people to express themselves.
Transsexual – a person who identifies as a member of the ‘opposite’ sex (ie. other than their birth sex) who usually seeks hormone therapy and often surgery to bring their body into line with their gender identity. Transsexual is an older term, and unlike transgender, is not an umbrella term. Many transgender people do not identify as transsexual.
Transgender female or Trans woman – a person who was assigned male at birth who identifies as female/woman.
Transgender male or Trans man – a person who was assigned female at birth who identifies as a male/man.
Brotherboy – Brotherboy and Sistergirl are terms used by transgender people within some Aboriginal and Torres Strait Islander communities. Brotherboys are Aboriginal and Torres Strait Islander men who were classified female at birth but live their lives as men.
Sistergirl – Brotherboy and Sistergirl are terms used by transgender people within some Aboriginal and Torres Strait Islander communities. Sistergirls are Aboriginal and Torres Strait Islander women who were classified male at birth but live their lives as women, including taking on traditional cultural female practices.
Affirming gender – a personal decision that involves a person seeking to redress a mismatch between their sex assigned at birth and their gender identity. A person living in their affirmed gender does not necessarily involve surgery.
Misgendering – a term for describing or addressing someone using language that does not match how that person identifies their own gender or body. For example, using the pronoun ‘he’ instead of ‘she’ to describe a trans woman.
Cisgender – a person who identifies with their sex assigned at birth.
Sex – refers to the biological characteristics of a person, which include chromosomes, hormones and reproductive organs.
Sex assigned at birth – refers to the sex category assigned to a person when they were born.
Gender diverse – a term which encompasses all gender identities and expressions that are different from a person’s sex assigned at birth. Includes people who identify as agender (having no gender), as bi-gender (both a woman and a man) or as non-binary (neither woman nor man), and some nonbinary people identify as genderqueer or as having fluid genders.
Transgender or Trans – a person whose gender identity does not align with their sex assigned at birth. Trans is an umbrella term that includes a wide variety of identities. Not everyone who falls under this umbrella refers to themselves as ‘trans’. For example, while some women who have transitioned or affirmed their gender may refer to themselves as trans women, others may simply refer to themselves as women, and others will use a variety of terms. There is no one ‘correct’ or ‘complete’ way for people to express themselves.
Transsexual – a person who identifies as a member of the ‘opposite’ sex (ie. other than their birth sex) who usually seeks hormone therapy and often surgery to bring their body into line with their gender identity. Transsexual is an older term, and unlike transgender, is not an umbrella term. Many transgender people do not identify as transsexual.
Transgender female or Trans woman – a person who was assigned male at birth who identifies as a female/woman.
Transgender male or Trans man – a person who was assigned female at birth who identifies as a male/man.
Brotherboy – Brotherboy and Sistergirl are terms used by transgender people within some Aboriginal and Torres Strait Islander communities. Brotherboys are Aboriginal and Torres Strait Islander men who were classified female at birth but live their lives as men.
Sistergirl – Brotherboy and Sistergirl are terms used by transgender people within some Aboriginal and Torres Strait Islander communities. Sistergirls are Aboriginal and Torres Strait Islander women who were classified male at birth but live their lives as women, including taking on traditional cultural female practices.
Affirming gender – a personal decision that involves a person seeking to redress a mismatch between their sex assigned at birth and their gender identity. A person living in their affirmed gender does not necessarily involve surgery.
Misgendering – a term for describing or addressing someone using language that does not match how that person identifies their own gender or body. For example, using the pronoun ‘he’ instead of ‘she’ to describe a trans woman.
Cisgender – a person who identifies with their sex assigned at birth.
Sex – refers to the biological characteristics of a person, which include chromosomes, hormones and reproductive organs.
Sex assigned at birth – refers to the sex category assigned to a person when they were born.
Intersex – people who are born with sex characteristics that don’t fit medical norms for female or male bodies. These characteristics can be physical, hormonal or genetic. People may describe themselves as intersex, or as having an intersex variation.
Sexual orientation
Sexual orientation – encompasses several dimensions of sexuality including sexual identity, attraction and behaviour, and refers to a person’s emotional, physical and/or sexual attraction to another person.
Sexual identity – self-identified label that a person may choose to describe themselves. For example, gay, lesbian or bisexual.
Gay/Homosexual – a person who experiences attraction (romantic, sexual, affectional, and/or emotional) solely or primarily to people of the same gender. Although it may be used by people of all genders, it is more commonly used by men.
Lesbian – a woman who experiences attraction (romantic, sexual, affectional, and/or emotional) solely or primarily to other women.
Bisexual/Pansexual – a person who experiences attraction (romantic, sexual, affectional, and/or emotional) to more than one gender. People who are pansexual may seek to express that gender does not factor into their own sexuality, or, that they are specifically attracted to trans, genderqueer, and other people who may or may not fit into the binary gender categories of male and female. This does not mean, however, that people who identify as bisexual are fixated on traditional notions of gender.
Queer – a term used by some people whose identity is not adequately described by existing categories or labels (such as lesbian, gay, or bisexual). It also extends outside of sexual orientation in that it is sometimes used as an umbrella term to include the diversity of sexual and/or gender identities in LGBTI communities. Some people prefer not to use this term as the history of the word has negative connotations, but in more recent times, the term has been reclaimed as a symbol of pride.
Asexual – people who do not experience sexual attraction, although this does not preclude romantic attraction.
Societal attitudes and issues
Biphobia – negative beliefs, prejudices and stereotypes that exist about people who are bisexual.
Homophobia – negative beliefs, prejudices and stereotypes that exist about people who are homosexual.
Intersexphobia or Interphobia – negative beliefs, prejudices and stereotypes that exist about intersex people.
Transphobia – negative beliefs, prejudices and stereotypes that exist about trans and gender diverse people.
Outing – threatening to disclose someone’s gender identity, sex, sexual orientation or intersex variation.
132 RCFV 2016, Volume 5 Report and recommendations, p.141.
133 Ibid.
134 Trans and gender diverse definition source, Transgender Victoria. Intersex definition source, Intersex Human Rights Australia. It is important to note that intersex is not a third sex (White paper – Making the Count: Addressing data integrity gaps in Australian standards for collecting sex and gender information, National LGBTI Health Alliance, 2016).
135 RCFV 2016, Volume 5 Report and recommendations, p.143.
136 Ibid p.144.
137 ANROWS 2014, Violence against women: Key statistics, viewed 22 June 2018, www.anrows.org.au/publications/fast-facts-0/violence-against-women-key-statistics
138 US National Coalition of Anti-Violence Programs 2018, Community Action Toolkit for Addressing Intimate Partner Violence Against Transgender People, viewed 20 June 2018, https://avp.org/ncavp/ncavp-toolkits/
139 Barking and Dagenham NHS 2008, Domestic Violence: A resource for gay & bisexual men, viewed 20 June 2018,
www.domesticviolencelondon.nhs.uk/uploads/downloads/DV-Resource_for_Gay_Men.pdf
140 RCFV 2016, Volume 5 Report and recommendations, p.154.
141 Victorian Equal Opportunity and Human Rights Commission (VEOHRC) 2015, Submission to the Royal Commission into Family Violence, no. 609, p.17, viewed 22 June 2018, www.rcfv.com.au/Submission-Review
142 Gay and Lesbian Health Victoria, Australian Research Centre in Sex, Health & Society, La Trobe University 2015, Family Violence and the LGBTI Community: Submission to the Victorian Royal Commission into Family Violence, no. 821, viewed 22 June 2018, www.rcfv.com.au/Submission-Review
143 No To Violence and safe steps Family Violence Response Centre 2015, safe steps Family Violence Response Centre and No To Violence joint submission: Family Violence and LGBTIQ Communities, no. 933, viewed 22 June 2018, www.rcfv.com.au/Submission-Review
144 Irlam, C B 2012, LGBTI Data: Developing an evidence-informed environment for LGBTI public policy, National LGBTI Health Alliance, Sydney.
145 No To Violence and safe steps Family Violence Response Centre 2015, safe steps Family Violence Response Centre and No To Violence joint submission: Family Violence and LGBTIQ Communities, no. 933, viewed 22 June 2018, www.rcfv.com.au/Submission-Review
146 Irlam, C B 2012, LGBTI Data: Developing an evidence-informed environment for LGBTI public policy, National LGBTI Health Alliance, Sydney.
147 RCFV 2016, Volume 5 Report and recommendations, p.142.
148 Irlam, C B 2012, LGBTI Data: Developing an evidence-informed environment for LGBTI public policy, National LGBTI Health Alliance, Sydney.
149 Attorney-General’s Department 2015, Australian Government Guidelines on the Recognition of Sex and Gender, viewed 20 June
2018, www.ag.gov.au/Publications/Pages/AustralianGovernmentGuidelinesontheRecognitionofSexandGender.aspx
150 Ibid.
151 ABS 2016, 1200.0.55.012 Standard for Sex and Gender Variables, 2016, viewed 20 June 2018,
www.abs.gov.au/ausstats/abs@.nsf/latestProducts/1200.0.55.012Media%20Release12016
152 Ansara, Y G 2016, Making the Count: Addressing data integrity gaps in Australian standards for collecting sex and gender information [White paper], National LGBTI Health Alliance, Newtown.
153 Ibid.
154 ABS 2016, 1200.0.55.012 Standard for Sex and Gender Variables, 2016, viewed 20 June 2018, www.abs.gov.au/ausstats/abs@.nsf/latestProducts/1200.0.55.012Media%20Release12016
155 The Sex and Gender Advisory Group consists of members from five Australian organisations; National LGBTI Health Alliance, A Gender Agenda, Intersex Human Rights Australia (formerly known as Organisation Intersex International Australia), Transformative and Transgender Victoria.
156 Ansara, Y G, Webeck, S, Carpenter, M, Hyndal, P & Goldner, S 2015, Re Commonwealth Attorney-General’s Department Review of the Australian Government Guidelines on the Recognition of Sex and Gender, LGBTI Health Alliance, Sydney.
157 Ibid.
158 Ansara, Y G 2016, Making the Count: Addressing data integrity gaps in Australian standards for collecting sex and gender information [White paper], National LGBTI Health Alliance, Newtown.
159 Statistics New Zealand 2015, Gender identity, viewed 20 June 2018, archive.stats.govt.nz/methods/classifications-andstandards/
classification-related-stats-standards/gender-identity.aspx
160 UK Office for National Statistics 2017, Gender identity update, viewed 20 June 2018, www.ons.gov.uk/methodology/classificationsandstandards/measuringequality/genderidentity/genderidentityupdate
161 ABS 2015, 4159.0 General Social Survey: Summary Results, Australia, 2014, viewed 20 June 2018, abs.gov.au/ausstats/abs@.nsf/mf/4159.0
162 Rainbow Health Ontario 2012, LGBTQ Research with Secondary Data [Fact Sheet], viewed 20 June 2018,
www.rainbowhealthontario.ca/resources/rho-fact-sheet-lgbt-research-with-secondary-data/
163 LGBT Foundation and NHS England 2017, Sexual Orientation Monitoring: Full Specification, viewed 20 June 2018,
www.england.nhs.uk/publication/sexual-orientation-monitoring-full-specification/
164 Ibid.
165 Misgendering is a term for describing or addressing someone using language that does not match how that person identifies their own gender or body. For example, using the pronoun ‘he’ instead of ‘she’ to describe a trans woman.
166 Gay and Lesbian Health Victoria, Australian Research Centre in Sex, Health and Society and La Trobe University 2016, The Rainbow Tick Guide to LGBTI-inclusive practice, La Trobe University, Melbourne.
167 Ansara, Y G, 2013, Inclusive Language Guide: Respecting people of intersex, trans and gender diverse experience, National LGBTI Health Alliance, Newtown.
168 State Government of Victoria 2016, Inclusive Language Guide, viewed 20 June 2018, https://www.vic.gov.au/equality/inclusivelanguage-guide.html
169 Ansara, Y G, 2013, Inclusive Language Guide: Respecting people of intersex, trans and gender diverse experience, National LGBTI Health Alliance, Newtown.
170 Ibid.
171 Ibid.
172 Ibid.
173 State Government of Victoria 2016, Inclusive Language Guide, viewed 20 June 2018, https://www.vic.gov.au/equality/inclusivelanguage-guide.html
174 AIFS 2017, LGBTIQ+ communities: Glossary of common terms, viewed 20 June 2018, https://aifs.gov.au/cfca/publications/lgbtiqcommunities
175 Australian Human Rights Commission 2011, Addressing sexual orientation and sex and/or gender identity discrimination: Consultation Report, viewed 20 June 2018, www.humanrights.gov.au/our-work/sexual-orientation-sex-gender-identity/publications/addressingsexual-
orientation-and-sex
176 VEOHRC 2014, Guideline: Transgender people at work – Complying with the Equal Opportunity Act 2010 in Employment, viewed 20 June 2018, www.humanrightscommission.vic.gov.au/our-resources-and-publications/eoa-practice-guidelines/item/632-guidelinetransgender-people-at-work-complying-with-the-equal-opportunity-act-2010
177 Strauss, P, Cook, A, Winter, S, Watson, V, Wright Toussaint, D & Lin, A 2017, Trans Pathways: the mental health experiences and
care pathways of trans young people, Telethon Kids Institute Australia, Perth.
178 Ansara, Y G, 2013, Inclusive Language Guide: Respecting people of intersex, trans and gender diverse experience, National LGBTI Health Alliance, Newtown.
179 Strauss, P, Cook, A, Winter, S, Watson, V, Wright Toussaint, D & Lin, A 2017, Trans Pathways: the mental health experiences and
care pathways of trans young people, Telethon Kids Institute Australia, Perth.
180 Transcend 2018, Terminology & Inclusive Language, viewed 20 June 2018, www.transcendsupport.com.au/terminology-inclusivelanguage/
181 National LGBTI Health Alliance 2016, National Lesbian, Gay, Bisexual, Transgender and Intersex Mental Health and Suicide
Prevention Strategy: A new strategy for inclusion and action, viewed 20 June 2018, lgbtihealth.org.au/wpcontent/uploads/2016/12/LGBTI_Report_MentalHealthandSuicidePrevention_Final_Low-Res-WEB.pdf
182 Transgender Victoria 2013, About TGV, viewed 20 June 2018, www.transgendervictoria.com/about.
183 Transcend 2018, Terminology & Inclusive Language, viewed 20 June 2018, www.transcendsupport.com.au/terminology-inclusivelanguage/
184 AIFS 2017, LGBTIQ+ communities: Glossary of common terms, viewed 20 June 2018, https://aifs.gov.au/cfca/publications/lgbtiqcommunities
185 Queensland Association for Healthy Communities Inc 2008, Supporting transgender and sistergirl clients: Providing respectful and inclusive services to transgender and sistergirl clients, viewed 20 June 2018, www.rainbowhealthontario.ca/resources/supportingtransgender-and-sistergirl-clients-providing-respectful-and-inclusive-services-to-transgender-and-sistergirl-clients/
186 Toone K, Sistergirls and the impact of community and family on wellbeing, honours thesis, Flinders University, Adelaide, viewed 20 June 2018, http://www.flinders.edu.au/
187 Balarajan, M, Gray, M & Mitchell, M 2011, Monitoring equality: Developing a gender identity question [Research Report], Equality and Human Rights Commission UK, Manchester.
188 Attorney-General’s Department 2015, Australian Government Guidelines on the Recognition of Sex and Gender, viewed 20 June
2018, www.ag.gov.au/Publications/Pages/AustralianGovernmentGuidelinesontheRecognitionofSexandGender.aspx
189 The Sex and Gender Advisory Group consists of members from five Australian organisations; National LGBTI Health Alliance, A Gender Agenda, Organisation Intersex International Australia, Transformative and Transgender Victoria.
190 Ansara, Y G, Webeck, S, Carpenter, M, Hyndal, P & Goldner, S 2015, Re Commonwealth Attorney-General’s Department Review of the Australian Government Guidelines on the Recognition of Sex and Gender, LGBTI Health Alliance, Sydney.
191 The Gender Identity in U.S. Surveillance Group 2014, Best Practices for Asking Questions to Identify Transgender and Other Gender Minority Respondents on Population-Based Surveys, the Williams Institute, Los Angeles.
192 Center of Excellence for Transgender HIV Prevention 2009, Recommendations for Inclusive Data Collection of Trans People in HIV Prevention, Care & Services, University of California, San Francisco.
193 Balarajan, M, Gray, M & Mitchell, M 2011, Monitoring equality: Developing a gender identity question [Research Report], Equality and Human Rights Commission UK, Manchester.
194 Peer Advocacy Network for the Sexual Health of Trans Masculinities 2017, Position Statement: Data Collection, viewed 20 June 2018, www.grunt.org.au/wp-content/uploads/PASH.tm-Data-Collection_Nov_2017.pdf
195 Cahill, S, Singal, R, Grasso, C, King, D, Mayer, K, Baker, K & Makadon, H 2014, ‘Do Ask, Do Tell: High Levels of Acceptability by Patients of Routine Collection of Sexual Orientation and Gender Identity Data in Four Diverse American Community Health Centers’, PLoS ONE, vol. 9, no. 9.
196 National LGBT Health Education Center, The Fenway Institute 2016, Collecting Sexual Orientation and Gender Identity Data in
Electronic Health Records: Taking the Next Steps, viewed 20 June 2018, http://www.lgbthealtheducation.org/wpcontent/
uploads/Collecting-SOGI-Data-in-EHRs-COM2111.pdf
197 Deutsch, M B, Green, J, Keatley, J, Mayer, G, Hastings, J & Hall, A M 2013, ‘Electronic medical records and the transgender patient: recommendations from the World Professional Association for Transgender Health EMR Working Group’, Journal of the American Medical Informatics Association, vol. 20, no. 4, pp. 700-703.
198 VEOHRC 2017, Guideline: Family violence services and accommodation – Complying with the Equal Opportunity Act 2010, viewed 20 June 2018, www.humanrightscommission.vic.gov.au/home/our-resources-and-publications/eoa-practice-guidelines/item/1577-guideline-family-violence-services-and-accommodation-complying-with-the-equal-opportunity-act-2010
199 Ansara, Y G 2016, Making the Count: Addressing data integrity gaps in Australian standards for collecting sex and gender information [White paper], National LGBTI Health Alliance, Newtown.
200 Irlam, C B 2012, LGBTI Data: Developing an evidence-informed environment for LGBTI public policy, National LGBTI Health Alliance, Sydney.
201 Australian Human Rights Commission 2011, Addressing sexual orientation and sex and/or gender identity discrimination: Consultation Report, viewed 20 June 2018, www.humanrights.gov.au/our-work/sexual-orientation-sex-gender-identity/publications/addressingsexual-
orientation-and-sex
202 Irlam, C B 2012, LGBTI Data: Developing an evidence-informed environment for LGBTI public policy, National LGBTI Health Alliance, Sydney.
203 LGBT Foundation and NHS England 2017, Sexual Orientation Monitoring: Full Specification, viewed 20 June 2018,
www.england.nhs.uk/publication/sexual-orientation-monitoring-full-specification/
204 DHHS 2018, Rainbow eQuality guide definitions, viewed 20 June 2018, https://www2.health.vic.gov.au/about/populations/lgbtiq-health/rainbow-equality/definitions
205 National LGBTI Health Alliance 2015, ‘LGBTI’ people and communities, viewed 20 June 2018, https://lgbtihealth.org.au
206 Bisexual Alliance Victoria Inc, About, viewed 20 June 2018, www.bi-alliance.org/?page_id=2
207 Bisexual.org 2013, What is the difference between bisexual and terms like pansexual, polysexual, omnisexual, ambisexual, and fluid?, viewed 20 June 2018, https://bisexual.org/?qna=what-is-the-difference-between-bisexual-and-terms-like-pansexual-polysexualomnisexual-ambisexual-and-fluid
208 LGBT Foundation 2017, Good Practice Guide to Monitoring Sexual Orientation, viewed 20 June 2018, https://s3-eu-west-1.amazonaws.com/lgbt-website-media/Files/b577e0cd-041a-4b10-89b6-f0f5f3384961/LGBTF%2520SOM%2520Report.pdf
209 Intersex Human Rights Australia (IHRA) 2014, We are Intersex Human Rights Australia, viewed on 20 June 2018, ihra.org.au
210 Organisation Intersex International Australia 2014, Making your service intersex friendly, viewed 21 June 2018, https://ihra.org.au/services/
211 Ansara, Y G 2016, Making the Count: Addressing data integrity gaps in Australian standards for collecting sex and gender information [White paper], National LGBTI Health Alliance, Newtown.
212 IHRA 2012, Including intersex in research studies and surveys, viewed 21 June 2018, ihra.org.au/20042/on-requests-for-research/
213 AIFS 2017, LGBTIQ+ communities: Glossary of common terms, viewed 20 June 2018, https://aifs.gov.au/cfca/publications/lgbtiqcommunities
214 Ansara, Y G 2013, Inclusive Language Guide: Respecting people of intersex, trans and gender diverse experience, National LGBTI Health Alliance, Newtown.
215 Australian Human Rights Commission 2011, Addressing sexual orientation and sex and/or gender identity discrimination: Consultation Report, viewed 20 June 2018, www.humanrights.gov.au/our-work/sexual-orientation-sex-gender-identity/publications/addressingsexual-
orientation-and-sex
216 Irlam, C B 2012, LGBTI Data: Developing an evidence-informed environment for LGBTI health policy. National LGBTI Health Alliance, Sydney.
217 Strauss, P, Cook, A, Winter, S, Watson, V, Wright Toussaint, D & Lin, A 2017, Trans Pathways: the mental health experiences and
care pathways of trans young people, Telethon Kids Institute Australia, Perth.
218 VEOHRC 2014, Guideline: Transgender people at work – Complying with the Equal Opportunity Act 2010 in Employment, viewed 20 June 2018, www.humanrightscommission.vic.gov.au/our-resources-and-publications/eoa-practice-guidelines/item/632-guidelinetransgender-people-at-work-complying-with-the-equal-opportunity-act-2010
219 Smith, E, Jones, T, Ward, R, Dixon, J, Mitchell, A & Hillier, L 2014, From Blues to Rainbows: Mental health and wellbeing of gender diverse and transgender young people in Australia, The Australian Research Centre in Sex, Health, and Society, Melbourne.
220 Organisation Intersex International Australia 2014, Making your service intersex friendly, viewed 21 June 2018, https://ihra.org.au/services/
221 National LGBTI Health Alliance 2015, LGBTI people and communities, viewed 20 June 2018, lgbtihealth.org.au/communities
222 Transgender Victoria 2013, Definitions, viewed 20 June 2018, www.transgendervictoria.com/about/definitions
223 Transcend 2018, Terminology & Inclusive Language, viewed 20 June 2018, www.transcendsupport.com.au/terminology-inclusivelanguage
224 DHHS 2018, Rainbow eQuality guide definitions, viewed 20 June 2018, https://www2.health.vic.gov.au/about/populations/lgbtiq-health/rainbow-equality/definitions
225 Bisexual Alliance Victoria Inc, viewed 20 June 2018, www.bi-alliance.org
226 The University of Western Australia, Sexuality and gender terms, viewed 20 June 2018, student.uwa.edu.au/experience/health-wellbeing-safety/fit/share/sexuality/definitions
227 IHRA website, viewed 20 June 2018, https://ihra.org.au
Data collection standards - People with disabilities
This section of the framework highlights the unique forms of family violence perpetrated against people with disabilities and the difficulties experienced responding to or reporting family violence incidents.
People with disabilities were recognised by the RCFV as a priority community affected by family violence. This section of the framework highlights the unique forms of family violence perpetrated against people with disabilities and the difficulties experienced responding to or reporting family violence incidents. It is noted that there are limitations which exist in current data standards, and that available administrative data concerning people with disabilities and their experiences of family violence are limited. This section contains data items recommended for use to ensure the consistent and accurate collection of disability information by organisations who respond to or provide services for family violence incidents.
Terminology and definitions
While there are many terms which can be used to describe people with disabilities, it is widely accepted that people-first language228 is favoured. However, there is some debate as to whether disability should be expressed in its singular or plural form.229 The framework will use the term ‘people with disabilities’, as this term is used in the RCFV report, and is recommended by the Judicial College of Victoria in their Disability Access Bench Book.230
Disability is a complex and evolving concept, and there is no standard definition of disability used across all government agencies and services. The DHHS Disability Action Plan 2018-2020231 defines people with disability as a diverse group, with a shared experience of encountering negative attitudes and barriers to full participation in everyday activities. The Disability Action Plan outlines that some conditions and impairments are present from birth and in other cases, people acquire or develop a disability during their lifetime from an accident, condition, illness or injury. The action plan acknowledges that some people are said to have dual disability. In their standard set of questions to capture information on disability, the AIHW defines disability as “a general term that covers:
- impairments in body structures or functions (for example, loss or abnormality of a body part)
- limitations in everyday activities (such as difficulty bathing or managing daily routines)
- restrictions in participation in life situations (such as needing special arrangements to attend work)”232
The AIHW definition informs national existing data standards for the collection of disability information, and this framework draws on those national standards.
| Legislative definitions of disability |
|---|
| State and Commonwealth legislation include various definitions of disability. These definitions range from broad (for example, the Equal Opportunity Act 2010 (Vic)) to specific (for example, the Guardianship and Administration Act 1986 (Vic)). Please note that this framework may not identify individuals who meet a specific legislative definition of disability. If an office or agency is required to identify people with disabilities in response to legislation which has a narrow definition of disability, they may need to collect additional information from clients beyond what is included in this standard to meet their specific internal needs. |
| How does mental illness relate to disability? |
|---|
| Psychosocial disability is a term used to describe individuals living with a disability that is associated with a severe mental illness.233 It is important to note that not all people with a mental illness will experience psychosocial disability,234 and although mental illness may overlap with experiences of disability, it is not often considered a disability in its own right. This section of the framework will discuss mental illness from the context of a psychosocial disability, and data items included in this standard only concern the collection of mental illness information where it is a source of disability. Agencies and service providers seeking to collect information on mental illness from a broader context than disability are encouraged to review existing national standards (for example, METeOR identifier: 399750 – Person identified with a mental health condition indicator).235 |
Family violence and people with disabilities
The RCFV report and research provides detailed information regarding what is known about the experiences of family violence faced by people with disabilities, and recommendations to address these issues. Summarised below are key points regarding the prevalence and issues stemming from family violence impacting this community.
Prevalence
Research and evidence presented to the RCFV suggested that people with disabilities are more often subjected to family violence compared with the general population. Although data in Australia are limited, research highlighted by the Australian Human Rights Commission found that nearly half of women with a disability surveyed in the UK reported having experienced domestic violence in their lives.236 In their research paper ‘Voices against Violence (paper 1)’, Women with Disabilities similarly acknowledged that international research indicates that women with disabilities are at a heightened risk of experiencing family and sexual violence compared to women without disabilities.237
The Human Rights Commission noted that a national survey of 367 family violence agencies found that approximately 22% of women and children accessing services were recorded as having a disability. While this number does not account for women with disabilities who do not access family violence services, it does support the position that this population is at a heightened risk for family violence victimisation in Australia.
Contributing circumstances and specific presentations of family violence risk
Family violence incidents are often understood to occur within relationships characterised by coercion, control and domination. It was noted by the RCFV that when perpetrators are in a position of power within a relationship, there is a higher occurrence of family violence.238 Due to social and environmental barriers, people with disabilities may more often be in a position of inequality with others, which in turn increases their risk of abuse. In their submission to the RCFV, the Office of the Public Advocate stated that “[w]hile women with disabilities experience many of the same forms of violence that other women experience, what they experience may be particular to their situation of disadvantage, cultural devaluation and increased dependency on others”.239
The RCFV found that when people with disabilities are dependent upon others for assistance they are:
- more likely to experience family violence240
- more likely to be abused by a wide range of perpetrators (including intimate partners, family members and caregivers)241
- more likely to be exposed to a wide range of abuses (including abuses which exploit a person’s need for assistance, such as withholding access to medication)242
- less likely to report family violence to others.243
Under-reporting and barriers to accessing services
Most crimes against people with disabilities go unreported, largely because of multifaceted barriers which prevent or discourage them from reporting crime.244 Under-reporting of family violence incidents involving people with disabilities is typically explained by the environmental, social and personal factors which impact a person’s decision to either not disclose incidents of family violence, or, when family violence is reported, to withhold information about their disability. In order to improve the quality of administrative data which exists in Victoria concerning people with disabilities impacted by family violence, barriers to reporting must be addressed.
Some of the reasons that people with disabilities may not disclose a family violence incident, or not access family violence services include:
- fear of discrimination or discriminatory treatment
- lack of knowledge about what constitutes family violence, who to report to and how the report can be made
- fear they will not be believed or viewed as credible
- fear that the abuse will be minimised or not taken as seriously as it should be
- reluctance to disclose stemming from past experiences of how people with disabilities have been treated by police and government agencies, including having been restrained or placed in involuntary care
- an inability to use oral or written language to communicate the details of a family violence incident in a way that is required by a person collecting data
- poor physical access to services, including building access restrictions, and limited phone and technology access
- concerns regarding the consequences of reporting. For example, if a person is physically dependent on the perpetrator, they may worry about that person being removed if no other care arrangement can be made. Similarly, if the person reports and nothing is done, the abuse may worsen.
Why do we need to collect information on disability?
The need to collect data on disability by family violence service providers and agencies was noted by the RCFV, with recommendation 170 stating that “the Victorian Government adopt a consistent and comprehensive approach to the collection of data on people with disabilities who experience or perpetrate family violence”.245 In Victoria, there is currently minimal available information on people with disabilities and their experience with family violence. Without adequate data on the subject, it is difficult to make informed decisions about service demand, intervention strategies and risk factors associated with future exposure to family violence.
Limited available data
A major concern highlighted by the RCFV was the absence of national level data which can be used to understand the prevalence of family violence impacting people with disabilities. One of the best sources of survey data in Australia concerning family violence is the ABS Personal Safety Survey (PSS). The PSS collects information from men and women aged 18 and older about the nature and extent of violence experienced since the age of 15. While the survey contains valuable information on family violence in Australia, a small sample size limits the amount of information which can be collected. The survey currently captures information about disability status in addition to intimate partner violence, stalking, emotional abuse and physical and sexual abuse, however it notably does not collect information about many forms of family violence disproportionately experienced by people with disabilities, including family violence that is perpetrated by parents, children, or familial-like individuals, such as carers. In addition, the PSS does not offer assistance for people with communications disabilities to complete the survey, so this population is excluded from the data collection. As such, it is difficult to get a full picture from this survey about the impact of family violence on people with disabilities.
There is also an absence of administrative data available concerning people with disabilities and their experience with family violence. It was found that the lack of existing data can largely be attributed to the significant barriers people with disabilities face when seeking to report family violence,246 and inadequate data collection practices employed by agencies and service providers.247 In order to improve the collection of data on people with disabilities, attention should be directed to both reducing the barriers that people with disabilities face when reporting an incident, and improving the practices used by agencies and services for collecting disability information.
Operational need to identify disability and provide reasonable adjustments
People with disabilities may face significant barriers which impact their ability to access an agency or service. Under the Equal Opportunity Act 2010 (Vic) there is a duty for organisations “to take reasonable, proportionate and proactive steps towards eliminating discrimination”.248 Organisations should therefore be actively identifying people with disabilities in order to fulfil an operational need to offer appropriate accommodations where required. Failure to provide such adjustments may be determined to constitute indirect discrimination against a person with a disability.
Indirect discrimination is described in the Equal Opportunities Act 2010 (Vic) to occur when: “a person imposes, or proposes to impose, a requirement, condition or practice –
(a) that has, or is likely to have, the effect of disadvantaging people with an attribute and
(b) that is not reasonable”.249
An example of indirect discrimination includes a requirement that all people, without exception, wishing to file a complaint or grievance must do so in writing. This indirectly discriminates against those who are unable to write.
Challenges in current data collection practices
In the 2017 ‘Australia’s Welfare’ report, the AIHW noted that most non-disability specific services in Australia do not collect information on whether a person has a disability.250 When these services include the option to collect disability information, very often the associated questions are either not asked or responses are not recorded.
There are a number of explanations for inconsistent collection of disability information by agencies and service providers in Victoria. The lack of a consistent definition of disability across Australia, and the fragmented structure of disability supports and services, present a problem for standardised and comprehensive reporting of disability data. The National Disability Insurance Scheme (NDIS), National Disability Agreement, and state governing bodies all provide definitions of disability.251 As a result, the scope and detail of disability information collected may not be consistent across services. In addition, different types of services will collect different information depending on what is most relevant for service provision. For example, medical services may be more likely to collect disability information by way of diagnoses and medical history, while non-disability specific services may be more interested in collecting information concerning support needs or a need for reasonable adjustments.
A further barrier for the collection of consistent data may be that people with disabilities are reluctant to disclose their disability to service providers. This is due in part to a history of discrimination, people may also feel a service will not be able to help them if they disclose their disability.
Organisational culture, training and policies also play a role in the absence of administrative data concerning people with disabilities and their experience with family violence. This can include that the collection of disability information is not seen as a core business function, or that staff are reluctant or unsure of how best to collect disability information for fear of causing offence.
Existing data standards
In recent years there has been a push to ensure that the needs of people with disabilities when interacting with services and programs in Australia are addressed. In particular, the National Disability Strategy (NDS) 2010-2020 encourages improvements in performance by non-disability specific services in delivering outcomes for people with disabilities. A key first step in ensuring that services are more responsive to the needs of people with disabilities is to reliably and consistently identify individuals who may require accommodations. Additionally, the NDS recognises that “[g]ood data and research are especially necessary for a sound evidence base to improve the effectiveness of mainstream systems for people with disability”.252 As a result, there has been a national movement towards the creation and adoption of a standardised collection method to be used by services nationally to produce reliable and comparable data concerning people with disabilities.
Australian Bureau of Statistics
The Survey of Disability, Ageing and Carers (SDAC)
Currently, the main survey used by the ABS to collect information on disability in Australia is the Survey of Disability, Ageing and Carers (SDAC) which is designed to collect “information about the wellbeing, functioning and social and economic participation of people with disabilities in Australia”.253 The SDAC collects a comprehensive range of information about people with disabilities, but the level of detail and number of questions included in the survey is higher than what would be practical for use in an administrative setting.
The Supplementary Disability Survey (SDS)
In 2016, the ABS trialled a Supplementary Disability Survey (SDS), which is a short set of disability questions designed by the Washington Group on Disability Statistics, a branch of the United Nations Statistical Commission. This set of questions is known as the Washington Group Short Set, and was created to address an urgent need for internationally comparable data on disability.
The questions focus on limitations and impairments experienced in six domains. For each domain, respondents are asked to identify the level of impairment they face. The domains and impairment levels are described in the tables below.
| Domains |
|---|
| (1) Seeing |
| (2) Hearing |
| (3) Walking |
| (4) Cognition |
| (5) Self-care |
| (6) Communication |
| Measurement of difficulty |
|---|
| (a) No difficulty |
| (b) Some difficulty |
| (c) A lot of difficulty |
| (d) Cannot do at all |
Advantages of the SDS are that it is an internationally comparable standard, and it was designed with brevity, simplicity, and an ability to identify individuals with disabilities from a broad range of nationalities and cultures. However, the ABS found that the results of the SDS did not provide comprehensive information on disability, were not comparable with the SDAC, and the questions were not suitable for identifying intellectual or psychological disabilities or young children with disabilities.254
Australian Institute of Health and Welfare: Standardised Disability Flag Module
In 2012-13, the AIHW was tasked to design a short set of questions to be used nationally by all nondisability specific services to identify individuals with a long-term health condition or disability who report an activity limitation, a specific education participation restriction and/or a specific employment participation restriction.
The AIHW standardised disability flag module (the flag)255 (METeOR Identifier: 521050) is based on the International Classification of Functioning, Disability and Health, a classification of health domains put forward by the World Health Organisation, and is also consistent with surveys used by the ABS for collecting information on disability. It is intended for use across a wide range of sectors, enabling nationally consistent collection of information used to identify people with disabilities or long term health conditions who experience difficulties or need assistance in various areas of their life.
The flag’s questions can fit into an organisation’s typical process of collecting administrative data, whether this be the completion of a digital or paper form, or by staff interviewing a client or their proxy. The flag is comprised of three groups of questions:
- activity and participation need for assistance cluster (METeOR identifier: 505770)
- education participation restriction indicator (METeOR identifier: 520889)
- employment participation restriction indicator (METeOR identifier: 520912)
The flag is comprised of 10 mandatory questions which fall into one of the above groups. Responses concerning activity participation and need for assistance consist of eight questions which are recorded on a four point scale, ranging from ‘have no difficulty’ to ‘always/sometimes need help or supervision’. Questions concerning education and employment participation restrictions are asked separately and require a yes/no response.
Activity and participation need for assistance cluster (METeOR identifier: 505770)256
These questions are about whether you have any long-term health conditions or disabilities. A longterm health condition is one that has lasted, or is expected to last, 6 months or more. Examples of long-term health conditions that might restrict your routine activities include severe asthma, epilepsy, mental illness, hearing loss, arthritis, depression, autism, kidney disease, chronic pain, speech impairment or stroke.
| Choose one answer for each row | Always sometimes need help or supervision | Have difficulty but don’t need help and/or supervision | Don’t have difficulty but use aids/equipment/medication | Have no difficulty |
|---|---|---|---|---|
| Self-care e.g. showing or bathing; dressing or undressing; toileting; eating food. | □ | □ | □ | □ |
| Mobility e.g. moving around the house; moving around outside the home; getting in or out of a chair; using public transport. | □ | □ | □ | □ |
| Communication e.g. understanding or being understood by other people, including people you know; using a telephone. | □ | □ | □ | □ |
| Managing things around the home e.g. getting groceries; preparing meals; doing washing or cleaning; taking care of pets. | □ | □ | □ | □ |
| Managing tasks and handling managing time; planning activities; coping with pressure or stressful situations. | □ | □ | □ | □ |
| Personal relationships e.g. making friends; meeting new people; showing respect to others; coping with feelings and emotions. | □ | □ | □ | □ |
| Community life e.g. participating in sports, leisure or religious activities; being part of a social club or organisation. | □ | □ | □ | □ |
Education participation restriction indicator (METeOR identifier: 520889)257
|
The next question is about whether a long-term health condition or disability affects your participation in education, including school or another educational institution (such as TAFE, university, or skills centre). Participation in education is considered to be affected if you:
Does a long-term health condition or disability affect your participation in education? □ Yes |
Employment participation restriction indicator (METeOR identifier: 520912)258
|
The next question is about whether a long-term health condition or disability affects your participation in work. Participation in work is considered to be affected if you:
Does a long-term health condition or disability affect your participation in work (paid and/or volunteering)? □ Yes |
Applying data standards to the collection of disability information in a family violence context
While standards exist in Australia for the collection of disability information in the context of particular administrative collections by mainstream organisations and in the collection of survey data, there is no standard designed specifically for mainstream agencies who are collecting information in response to a family violence incident. Services and agencies who respond to family violence can be considered distinct from many other organisations in that they are often interacting with people in a crisis situation who may be experiencing extreme distress or an immediate need for service. In these circumstances, asking a number of questions about a person’s disability or daily limitations may not always be realistic or practical. It is however important information to establish in order to know how to appropriately respond to the person experiencing the family violence. Although the AIHW flag is recommended for use as the national standard for collecting information on disability, an abridged set of disability questions is also presented in this section for agencies and services who cannot practically implement the AIHW flag.
Data collection standard for collecting disability information
When collecting information about disability it is recommended that data collectors explain why the information is being collected, and ask if the client is comfortable answering questions about their health or disability. If a disability is disclosed, this should signal that a direct service response or referral to an appropriate service may be required.
It is recommended that service providers and agencies ask a person if they would like assistance to answer questions. This may include having a support person who can assist them (provided that this person is not the perpetrator or known by the perpetrator).
This data collection standard may have limitations for collecting information from certain people including those from different cultural backgrounds or experiences, or people with cognitive disabilities. Staff collecting information using this standard should therefore be mindful of the information being collected, including what it will be used for and when the collection methods should be altered to adjust for people who are from different cultures or have unique communication needs. More information can be found under ‘Considerations when implementing data items’ on page 81.
Agencies and services should note that questions about disability and health information are considered to be private information, and relevant privacy legislation, including the Health Records Act 2001 (Vic) and the Privacy and Data Protection Act 2014 (Vic) should be considered by data custodians when collecting and storing this information. Information concerning privacy and security considerations is discussed on page 18.
Overview of data collection standard
The disability standard proposed in this framework contains two components; ‘difficulty experienced and need for assistance’ and ‘disability group’. These two components contain data items which can be used to derive METeOR outputs. Agencies and services can use these outputs to identify whether a person has an activity limitation, the extent of their limitation, and to provide information about the disability group.
Difficulty experienced and need for assistance
This component collects information on difficulty experienced by a person and their need for assistance with employment, education and routine activities. This information can be gained either through use of the AIHW flag, or through the abridged disability set. Responses from either of these data collection sets can be used to derive METeOR data items as outputs, which provide information on whether a person experiences an activity limitation or participation restriction, and the extent of this limitation or restriction.
Disability group
This question asks respondents which response option(s) best describe the group(s) responsible for an impairment of body structure or function, limitation in activity or restriction in participation. Outputs from this component will provide more details about a person’s experience of disability, and may be used to flag for conditions which are of interest for research purposes, including acquired brain injuries.
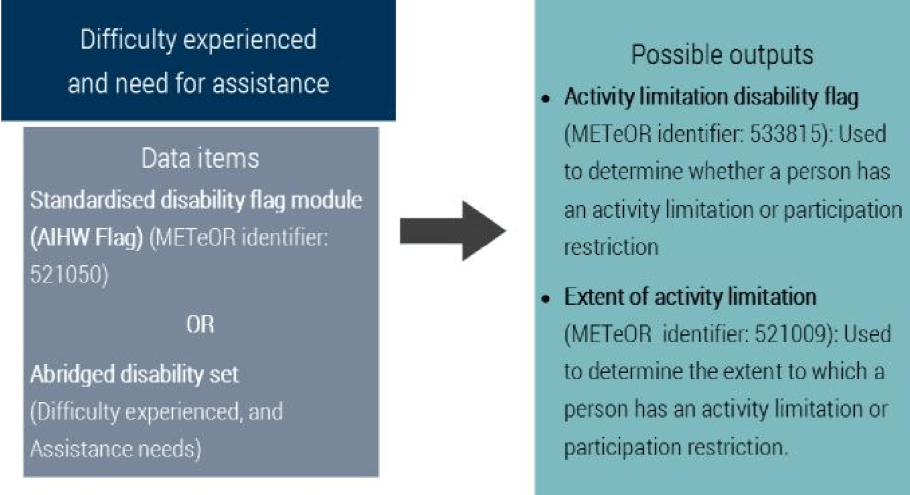
Abridged disability set
Where it is not practicable for a service or agency to use the AIHW flag, the abridged set of questions below is recommended. These two questions relate to the difficulty experienced by an individual and their assistance needs.
Difficulty experienced – Question phrasing and response categories
|
Because of a long-term health condition, mental illness or disability lasting or expected to last 6months or longer, do you experience any difficulty or restriction which affects your participation in activities at work, school1 or when doing routine tasks2? □ Yes 1. School refers to a range of educational institutions, including University, TAFE and other learning centres. 2. Routine tasks include bathing, dressing, eating, moving around the house or outside the home, communicating with others, making decisions, learning new things, preparing meals, managing daily routine, caring for children or others, coping with stress, making new friends or socialising with others. |
Assistance needs – Question phrasing and response categories
|
Because of a long-term health condition, mental illness or disability lasting or expected to last 6 months or longer, when at work, school or doing routine tasks, which of the following options best describes your need for assistance? □ Always/sometimes need help or supervision |
Using and interpreting responses
The ‘difficulty experienced’ and ‘assistance needs’ questions should be collected together in order for agencies and services to gather meaningful information about a person’s experience of disability or activity limitation. The results of these questions may be mapped to METeOR outputs. For information on how these response options can be mapped, please see ‘How to map responses from the abridged disability set to METeOR data items’ on the following page.
Disability group
This data item has been modified from the AIHW Disability group code (METeOR identifier: 680763).259 The advantage of using this question is that it captures additional information on disability, which is important for research and evaluation purposes. For instance, the RCFV identified that people with acquired brain injuries were a priority for research efforts concerning family violence, with current available information indicating that this group may be at an increased risk for using and experiencing family violence.
For this data item, the option to select multiple categories is strongly recommended. It is noted that some data collection systems may not be able to currently accommodate for multiple categories to be selected, however it is encouraged that service providers look into options for collecting multiple responses for disability group. People with disabilities often have comorbid conditions and may find it difficult to choose only one category which primarily causes impairments to their routine activities. If it is not possible to allow individuals to select multiple categories of disability, respondents should be asked to select the category which primarily causes the most difficulty for them in daily life.
It should be noted that this data item is not suitable for use on its own to collect information about disability. This question should be used in combination with the AIHW flag or the abridged disability set in order to collect information about disability.
Question phrasing and response categories
|
Do you have a long-term health condition or disability which can be described under the following categories? □ Intellectual (including Down syndrome) |
Using and interpreting responses
Responses from this data item can be used in combination with the previous data items used to collect information about the difficulty a person experiences and their need for assistance in order to provide detailed information about a person’s experience of disability.
When collecting data verbally, information and guidance should be provided to assist a respondent in understanding the response categories. Definitions can be found in the glossary at the end of this section.
How to map responses from the abridged disability set to METeOR data items
If an agency or service uses the abridged disability set rather than the AIHW flag, responses can be mapped to existing METeOR data items. The following figure describes how responses from the abridged disability set can be used to derive the response options included in the METeOR data items ‘derived activity limitation flag’, and ‘derived extent of activity limitation.’
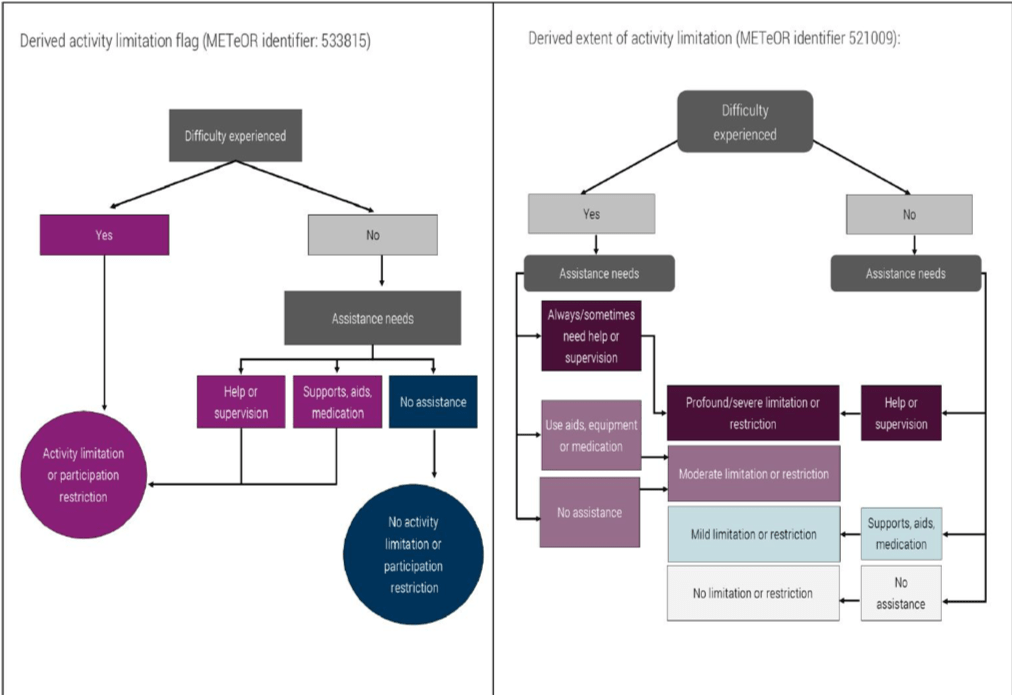
Reasonable adjustment question [optional but recommended]
Although this question is not part of the data collection standard and will not directly capture information about disability, it is recommended for use by service providers, particularly when clients or respondents have disclosed that they face difficulties on account of a disability. Organisations in Victoria are obligated under the Disability Discrimination Act 1992 (Cth) and the Equal Opportunity Act 2010 (Vic) to provide reasonable adjustments when needed for people with disabilities to access their services.
As many services will have ongoing communication with people accessing their services, this question asks if any adjustments need to be made regarding how an organisation communicates with a client. A service or agency should also ask other questions about reasonable adjustments which are specific to the services that they provide, for example, whether someone requires mobility assistance. The Australian Human Rights Commission’s factsheet ‘Access for all: improving accessibility for consumers with disability’ is a good resource for agencies or services looking to improve accessibility for people with disabilities.260
|
How should we communicate with you? □ Verbal communication |
Considerations when implementing data items
Data collectors should be mindful when questioning people with certain communication needs or people from different cultural backgrounds, that additional discussion may be needed to gain accurate information about disability. Administrative collection of disability information typically involves organisations asking close-ended questions about a person’s health and functioning. While this method is ideal for generating easily reportable data, it may present problems when collecting information from certain audiences. The following information highlights population groups who may benefit from the use of alternative wording or collection methods when asking about disability information, and the proper terminology to use when discussing concepts surrounding disability.
People who require assistance to communicate
People with disabilities who have difficulty communicating are especially at risk of not reporting incidents of family violence, largely because of the communication barriers they face when attempting to seek help. If an agency or service provider finds that they cannot communicate with a person with a disability through their normal business communication practice, then they should explore other methods which can be used to communicate with that person. Service providers should also be mindful to offer multiple communication options for people with disabilities when collecting information, including offering options for verbal communication, written communication, or communicating through an agreed third party.
People with a cognitive disability or need for easy English
Cognitive disability is a term used to describe a wide variety of impaired brain functions including impairment in comprehension, reasoning, adaptive functioning, judgement, learning or memory that
is the result of any damage to, dysfunction, developmental delay, or deterioration of the brain or mind.261 Cognitive disability can be used to incorporate a number of conditions, such as intellectual disability, acquired brain injuries, autism and dementia. People with a cognitive disability may have difficulty learning and recalling skills, following instruction, recognising cause and effect, or performing physical and cognitive tasks. Part of providing a more accessible service for people with a cognitive disability may include the use of easy English. Easy English is specifically designed to make sense to people who have difficulty reading and understanding English. It is a style of writing that is simple and concise, focuses on presenting key information rather than the detail, and uses a mix of words and images to enhance the message for the reader.262 Style guides and fact sheets can be found on the Scope website, www.scopeaust.org.au/service/accessible-information/.
Aboriginal and Torres Strait Islander people
People from Aboriginal or Torres Strait Islander communities may require alternative wording or additional conversation surrounding the concepts of disability, mental illness or medical conditions. While Aboriginal and Torres Strait Islander views on disability vary between different people, environments and cultures, there are some general concepts which may be relevant to discussions surrounding disability data collection by service providers. In their report entitled ‘Cultural Proficiency in Service Delivery for Aboriginal People with a Disability’, the NDS noted several barriers which may impact a person of Aboriginal or Torres Strait Islander origin from disclosing disability information. These include:263
- In certain traditional Aboriginal or Torres Strait Islander cultures, people with medical conditions or physical impairments are not viewed as distinct from the general population. Individuals from these communities may not have comparable concepts to assist with understanding disability as it is viewed in a Western context.
- Many people of Aboriginal or Torres Strait Islander origin experience discrimination, and may therefore be reluctant to have a second label applied to them which can be further prone to discrimination or discriminatory treatment.
- Some traditional Aboriginal communities view disability as a consequence of being ‘married the wrong way’. In these cases, disability may be a source of stigma or shame related to a ‘bad karma’ view of disability.
Additionally, the First Peoples Disability Network have emphasised that health for Aboriginal peoples focuses not only on physical health, but also encompasses spiritual, cultural, emotional and social wellbeing.264 Health is therefore more than the absence of sickness, but involves the relationship with family and community, providing a sense of belonging and connection with the environment. This holistic definition of health varies from how disability is defined in the disability data collection standard used in the framework, and therefore responses gained from data collection may not represent how Aboriginal people view their own health and wellbeing.
If any of the above barriers appear to be relevant when questioning an Aboriginal person about disability information, it may be more useful to have an open-ended discussion about a person’s routine life activities and needs for assistance, rather than relying on close-ended questions about disability.
People from culturally and linguistically diverse backgrounds
It was revealed during consultation with service providers that people from culturally and linguistically diverse backgrounds may benefit from alternative wording or additional conversation surrounding the concepts of disability, mental illness or long-term medical conditions. In particular it was noted that recent immigrants to Australia and people with limited English may experience difficulty understanding complex questioning around their health, or their ability to perform routine tasks. Additionally, in some circumstances refugees and new immigrants to Australia may not have had much exposure to Westernised medical care, making it less likely for these people to have received a recognised medical diagnosis. As such, they may be unaware if they have a condition which would be considered a source of disability. Finally, it was noted that many cultures outside of Australia do not have comparable concepts around disability and mental illness, and questions about these concepts may be confusing or offensive. In these cases, open ended discussions may be beneficial in making a determination about a person’s need for assistance.
People with a psychosocial disability
As this data collection standard was designed to capture information about a wide range of disabilities, the wording used in the data items may not be intuitive to trigger the disclosure of a psychosocial disability, particularly in cases where a condition is episodic. When appropriate, data collectors can employ alternative wording when asking about disability status. This can involve explaining that a condition can be something that causes a person difficulty for certain periods of time, and not necessarily something that is experienced daily, or at a constant level of severity.
Inclusive language
When describing disability, language that respects all people as active individuals with control over their own lives should be used. Negative language, such as ‘suffers from depression’, ‘afflicted with Multiple Sclerosis’ or ‘confined to a wheelchair’, should be avoided,265 and neutral phrases like ‘person experiencing depression’ or ‘person who uses a wheelchair’ should be used instead. As mentioned at the beginning of this section, using person-first language, for example, ‘people with disabilities’ is also preferred to outdated and offensive terms like ‘disabled person’, ‘bi-polar person’, ‘handicapped’ or ‘the disabled’.266 This language reinforces the notion that the term disability describes the barriers that a person faces when engaging with their environment, and it does not define the characteristics of an individual. ‘Training and resources’, at the end of this section, outlines organisations in Victoria and nationally that provide advocacy, information, training and assistance for agencies or service providers working with people with disabilities.
Training and resources
Training and communication resources
Australian Sign Language Interpreters’ Association Victoria
The Victorian professional body for Auslan interpreters.
Website: www.asliavic.org.au
Email: info@asliavic.com.au
Beyond Blue
Provides information and support to help everyone in Australia achieve their best possible mental health. They can provide special resources and training for schools, workplaces, aged care and health professionals.
Website: www.beyondblue.org.au
Phone: 03 9810 6111
Communication Rights Australia
Communication Rights Australia provides advocacy and professional independent communication support worker (ICS) services.
Website: www.communicationrights.org.au
Phone: 03 9555 8552
Disability Advocacy Resource Unit
Provides training and resources to keep disability advocates informed and up to date about issues affecting people with disabilities in Victoria.
Website: www.daru.org.au
Phone: 03 9639 5807
Disability Justice Advocacy
Advocacy support for people with a disability in Victoria.
Website: www.justadvocacy.com
Phone: 03 9474 0077
Scope
Information and communication support services for people with complex communication needs. Scope can assist with developing communication aids and Easy English materials.
Website: www.scopevic.org.au
Phone: 1300 472 673
VicServ
The peak body for mental health services in Victoria.
Website: www.vicserv.org.au
Phone: 03 9519 7000
Victorian Mental Illness Awareness Council
The peak Victorian non-government organisation for people with lived experience of mental health or emotional issues. Part of their role is to provide education to the community about mental illness from the consumer perspective, and they engage in educational activities for service providers who work in clinical and community support sectors.
Website: www.vmiac.org.au
Phone: 03 9380 3900
Disability information and advocacy bodies
Amaze
Information about autism spectrum disorder.
Website: www.amaze.org.au
Phone: 03 9657 1600
Blind Citizens Australia
Information about people who are blind or have low vision.
Website: www.bca.org.au
Phone: 1800 033 660
Cerebral Palsy Support Network
Information about people with cerebral palsy.
Website: www.cpsn.org.au
Phone: 03 9478 1001
Down Syndrome Victoria
A membership organisation providing parents, families, professionals and friends of people with Down Syndrome with support, information and resources.
Website: www.downsyndromevictoria.org.au
Email: info@dsav.asn.au
First Peoples Disability Network
A peak organisation representing Aboriginal and Torres Strait Islander people living with disability.
Website: www.communicationrights.org.au
Phone: 03 9555 8552
Headspace
The National Youth Mental Health Foundation provides early intervention mental health services to 12-25 year olds, along with assistance in promoting young peoples’ wellbeing. Information and services for young people, their families and friends as well as health professionals can be accessed through their website, Headspace centres, online counselling service eheadspace, the Digital Work and Study Service and postvention suicide support program headspace School Support.
Website: www.headspace.org.au
Phone: 03 9027 0100
Mind Australia
One of the country’s leading community-managed specialist mental health service providers, supporting people dealing with the day-to-day impacts of mental illness, as well as their family, friends and carers.
Website: www.mindaustralia.org.au/about-mind
Phone: 1300 286 453
Sane
Support and information about mental health disabilities.
Website: www.sane.org
Helpline: 1800 18 7263
VicDeaf
Information and services for people who are deaf or hard of hearing and individuals and organisations working with people who are deaf or hard of hearing, including Auslan interpreting services.
Website: www.vicdeaf.com.au
Phone: 03 9473 1111
Vision Australia
A national provider of blindness and low vision services.
Website: www.visionaustralia.org
Phone: 1300 84 74 66
Women with Disabilities
Information and advocacy for women with disabilities.
Website: www.wdv.org.au
Phone: 03 9386 7800
Glossary
Activity: Describes the execution of one or more tasks that a person may need to perform as part of their daily life. Can include cognitive, emotional, communication, health care, household chores, meal preparation, mobility, property maintenance, reading or writing, self-care or transportation related tasks.
Activity limitations: Difficulties an individual may have in executing activities, which may vary with the environment. Activity is limited when an individual, in the context of a long-term health condition or disability, either has a need for assistance in performing an activity in an expected manner, or cannot perform the activity at all.267
Disability: Disability is a complex and evolving concept, and there is no standard definition. AIHW defines it is a general term that covers impairments in body structures or functions (for example, loss or abnormality of a body part), limitations in everyday activities (such as difficulty bathing or managing daily routines) or restrictions in participation in life situations (such as needing special arrangements to attend work).268 The DHHS disability Plan 2018-19 defines people with a disability as a diverse group with a common shared experience of encountering negative attitudes and barriers to full participation in everyday activities.269
Impairments: Problems in body function or structure such as organs, limbs and their components.270
Mental health problem: Describes the broad range of features that interfere with how a person thinks, feels and behaves, but to a lesser extent than a mental illness. A person experiencing poor mental health therefore may not meet diagnostic criteria for a mental disorder, but may still experience a negative impact on their life.271
Mental illness: A clinical diagnosable illness that significantly interferes with an individual’s cognitive, emotional or social ability. The diagnosis of mental illness is generally made according to the classification systems of the ‘Diagnostic and statistical manual of mental disorders’ (DSM) or the ‘International classification of diseases’ (ICD).272
Psychosocial disability: A disability arising from a mental health issue.273
Reasonable adjustment: A modification made to the provision of a service in order to assist a person with an impairment to participate, access or derive benefit from that service. When determining whether an adjustment is reasonable or not, consult section 45(3) of the Equal Opportunities Act 2010 (Vic).
| Disability group |
|---|
|
The list below provides definitions for the response categories used in the ‘disability group’ data item on page 79. Intellectual: Applies to conditions appearing in the developmental period (0-18 years) and is associated with impairments of mental functions, difficulties in learning and performing certain routine activities, and limitations with adaptive skills in the context of community environments when compared with others of the same age. This category includes Down syndrome, tuberous sclerosis, Specific learning: Refers to learning disorders, including Attention Deficit Disorder, other than intellectual.275 Autism: Includes Asperger’s syndrome and Pervasive developmental delay.276 Physical: Used to describe conditions that are attributable to a physical cause or impact on the ability to perform physical activities, such as mobility. Physical disability often includes impairments of the neuromusculoskeletal systems including the effects of paraplegia, quadriplegia, muscular dystrophy, motor neuron disease, neuro muscular disorders, cerebral palsy, absence or deformities of limbs, spina bifida, arthritis, back disorders, ataxia, bone formation or degeneration and scoliosis.277 Acquired brain injury: Used to describe multiple disabilities arising from damage to the brain acquired after birth. Damage can result in deteriorated cognitive, physical, emotional or independent functioning. Causes include blunt force trauma, strokes, brain tumours, infection, poisoning, lack of oxygen and degenerative neurological disease.278 Neurological: Applies to impairments of the nervous system occurring after birth, and includes epilepsy and organic dementias (for example, Alzheimer’s disease), as well as conditions such as multiple sclerosis and Parkinson’s disease.279 Deafblind (dual sensory): Refers to a dual sensory impairment associated with severe restrictions in communication and participation in community life. Deafblindness is not just vision impairment with a hearing loss, or a hearing loss with a vision impairment. Deafblindness is a unique disability of its own requiring distinct communication and teaching practices.280 Vision: Encompasses blindness and vision impairment (not corrected by glasses or contact lenses), which can cause severe restriction in communication and mobility, and in the ability to participate in community life.281 Hearing: Encompasses deafness, hearing impairment and hearing loss.282 Speech: Encompasses speech loss, impairment and/or difficulty in being understood.283 Psychosocial: Includes an experience of disability associated with a mental illness.284 |
228 People-first language emphasises the person first, and not the disability. For example, using ‘person with a disability’, rather than ‘the disabled’.
229 People with Disability Australia 2017, Terminology used by PWDA, viewed 21 June 2018, www.pwd.org.au/studentsection/terminology-used-by-pwda.html
230 Judicial College of Victoria and VEOHRC 2016, Disability Access Bench Book, viewed 21 June 2018, www.judicialcollege.vic.edu.au/disability-access-bench-book
231 DHHS Disability Action Plan 2018-2020, https://dhhs.vic.gov.au/publications/disability-action-plan-2018-2020
232 AIHW Metadata Online Registry, Standardised disability flag module, viewed 21 June 2018, http://meteor.aihw.gov.au/content/index.phtml/itemld/521050
233 National Mental Health Consumer & Carer Forum (NMHCCF) 2011, Unravelling Psychosocial Disability, A Position Statement by the National Mental Health Consumer & Carer Forum on Psychosocial Disability Associated with Mental Health Conditions, NMHCCF, Canberra, p.9.
234 Ibid.
235 AIHW Metadata Online Registry, Person – formally diagnosed mental health condition indicator, code N, viewed 21 June 2018,
http://meteor.aihw.gov.au/content/index.phtml/itemld/399750
236 Ibid p.29.
237 Woodlock, D, Healey, L, Howe, K, McGuire, M, Geddes, V & Granek, S 2014, Voices Against Violence Paper One: Summary Report and Recommendations, Women with Disabilities Victoria, Office of the Public Advocate and Domestic Violence Resource Centre Victoria.
238 RCFV 2016, Volume 5 Report and recommendations, p.177.
239 Office of the Public Advocate 2015, Submission to the Victorian Royal Commission into Family Violence, no. 905, p.10, viewed 22
June 2018, www.rcfv.com.au/Submission-Review
240 RCFV 2016, Volume 5 Report and recommendations, p.177.
241 Ibid p.173.
242 Ibid.
243 Ibid p.183.
244 VEOHRC 2014, Beyond doubt: The experiences of people with disabilities reporting crime – Research findings, viewed 21 June 2018, www.humanrightscommission.vic.gov.au/our-resources-and-publications/reports/item/894-beyond-doubt-the-experiences-ofpeople-with-disabilities-reporting-crime.
245 RCFV 2016, Volume 1 Report and recommendations, p.90.
246 RCFV 2016, Volume 5 Report and recommendations, p.172.
247 VEOHRC 2014, Beyond doubt: The experiences of people with disabilities reporting crime – Research findings, viewed 21 June 2018, www.humanrightscommission.vic.gov.au/our-resources-and-publications/reports/item/894-beyond-doubt-the-experiences-ofpeople-with-disabilities-reporting-crime
248 VEOHRC, Positive duty, viewed 21 June 2018, www.humanrightscommission.vic.gov.au/home/the-law/equal-opportunity-act/positiveduty#what-is-the-positive-duty
249 Ibid.
250 AIHW 2017, Australia’s Welfare 2017, Australia’s welfare series no. 13, AIHW, Canberra, p.39.
251 Ibid.
252 Commonwealth of Australia 2011, National Disability Strategy 2010-2020, viewed 21 June 2018, www.dss.gov.au/ourresponsibilities/disability-and-carers/publications-articles/policy-research/national-disability-strategy-2010-2020
253 ABS 2016, 4430.0 Disability, Ageing and Carers, Australia: Summary of Findings, 2015, viewed 21 June 2018,
http://abs.gov.au/ausstats/abs@.nsf/Latestproducts/4430.0Main%20Features202015?opendocument&tabname=Summary&prodno=4430.0&issue=2015&num=&view
254 ABS 2016, 4450.0 Supplementary Disability Survey, 2016, viewed 21 June 2018, www.abs.gov.au/ausstats/abs@.nsf/mf/4450.0
255 The AIHW Data Collection Guide for use of the standardised disability flag module can be downloaded at www.aihw.gov.au/WorkArea/DownloadAsset.aspx?id=60129557264
256 AIHW Metadata Online Registry, Activity and participation need for assistance cluster (disability flag), viewed 21 June 2018,
http://meteor.aihw.gov.au/content/index.phtml/itemld/505770
257 AIHW Metadata Online Registry, Person – education participation restriction indicator, code N, viewed 21 June 2018,
http://meteor.aihw.gov.au/content/index.phtml/itemld/520889
258 AIHW Metadata Online Registry, Person – employment participation restriction indicator, code N, viewed 21 June 2018,
http://meteor.aihw.gov.au/content/index.phtml/itemld/520912
259 AIHW Metadata Online Registry, Disability group code N[N], viewed 21 June 2018, http://meteor.aihw.gov.au/content/index.phtml/itemld/680763
260 Australian Human Rights Commission 2016, Access for all: Improving accessibility for consumers with disability, viewed 21 June 2018, www.humanrights.gov.au/employers/good-practice-good-business-factsheets/access-all-improving-accessibility-consumers
261 Smith, M 2017, ‘Communicating effectively with people with cognitive disability’, paper presented at the Council of Australasian
Tribunals Conference, viewed 21 June 2018, http://www.coatconference.com.au/resources/Melinda%20Smith%20-%20PRESENTATION.pdf
262 Scope, Accessible Information and Easy English, https://www.scopeaust.org.au/service/accessible-information
263 National Disability Services 2014, Cultural Proficiency in Service Delivery for Aboriginal People with a Disability, viewed 21 June 2018, www.idfnsw.org.au/images/A_Guide_to_Cultural_Proficiency_in_Service_Delivery_for_Aboriginal_People_-_Information.pdf
264 First Peoples Disability Network Australia 2016, Intersectional Dimensions on the Right to Health for Indigenous Peoples – A Disability Perspective, http://www.disabilityjustice.edu.au/wp-content/uploads/2016/05/Intersectional-Dimensions-on-the-Right-to-Health-for-Indigenous-Peoples---A-Disability-Perspective-FPDN.pdf
265 Judicial College of Victoria and VEOHRC 2016, Disability Access Bench Book, viewed 21 June 2018, www.judicialcollege.vic.edu.au/disability-access-bench-book
266 Ibid.
267 Ibid.
268 AIHW Metadata Online Registry, Standardised disability flag module, viewed 21 June 2018, http://meteor.aihw.gov.au/content/index.phtml/itemld/521050
269 DHHS Disability Action Plan 2018-2020, https://dhhs.vic.gov.au/publications/disability-action-plan-2018-2020
270 World Health Organisation 2018, International Classification of Functioning, Disability and Health (ICF), viewed 21 June 2018,
www.who.int/classifications/icf/en/
271 Department of Health, National Mental Health Policy 2008: Glossary, viewed 13 June 2018, www.health.gov.au/internet/publications/publishing.nsf/Content/mental-pubs-n-pol08-3
272 National Mental Health Consumer & Carer Forum (NMHCCF) 2011, Unravelling Psychosocial Disability, A Position Statement by the National Mental Health Consumer & Carer Forum on Psychosocial Disability Associated with Mental Health Conditions, NMHCCF, Canberra, p.6.
273 National Disability Insurance Agency, Psychosocial disability, viewed 21 June 2018, ndis.gov.au/psychosocial/products
274 AIHW Metadata Online Registry, Disability group code N[N], viewed 21 June 2018, http://meteor.aihw.gov.au/content/index.phtml/itemld/680763
275 Ibid.
276 Ibid.
277 Ibid.
278 National Disability Services, Disability Types and Description, viewed 21 June 2018, www.nds.org.au/disability-types-anddescriptions
279 Ibid.
280 AIHW Metadata Online Registry, Disability group code N[N], viewed 21 June 2018, http://meteor.aihw.gov.au/content/index.phtml/itemld/680763
281 Ibid.
282 Ibid.
283 Ibid.
284 National Disability Insurance Agency, Psychosocial disability, viewed 21 June 2018, www.ndis.gov.au/psychosocial/products
Data collection standards - Culturally and linguistically diverse communities
Highlights the family violence issues faced by CALD communities, the challenges in collecting data from CALD communities, and existing data standards used to collect this information.
The RCFV highlighted that people from culturally and linguistically diverse (CALD) communities are disproportionately affected by family violence and face greater barriers to seeking assistance than those of an Anglo-Australian background.285 Despite Victoria being one of the most culturally diverse states in Australia, the collection of information about a person’s cultural background and language is inconsistent across agencies and service providers. This section of the framework highlights the family violence issues faced by CALD communities, the challenges in collecting data from CALD communities, and existing data standards used to collect this information. Data items are proposed for use in the collection of administrative data from CALD communities within the context of family violence.
Terminology and definitions
The phrase ‘culturally and linguistically diverse’ is a broad term used to describe communities with diverse languages, ethnic backgrounds, nationalities, traditions, societal structures and religions.286 This term is often used synonymously with the phrase ‘ethnic communities’, however, CALD is the preferred term used by Australian service providers and agencies.
A widely used definition of CALD refers to those people born overseas, in countries other than those classified by the ABS as ‘main English speaking countries’.287 The main English speaking countries identified by the ABS are Australia, Canada, Republic of Ireland, New Zealand, South Africa, United Kingdom (England, Scotland, Wales, Northern Ireland) and United States of America.288
While this is a commonly used definition, people born in these main English speaking countries may identify with another culture or country, and may still face language and other barriers when interacting with government departments and service providers.
CALD communities
|
This framework will use the definition from the RCFV and refer to CALD communities as people of non-English speaking background, as well as people born outside of Australia and whose first language is not English.289 People from faith-based communities can experience specific types of family violence, similar to those experienced in CALD communities. While people of various faiths may not be captured by |
The definition of CALD communities is intended to describe the characteristics of people who belong to these communities; not to determine whether a person ‘is CALD’. As outlined further in this section, a person’s cultural and linguistic diversity cannot be determined or summarised by one measure.
Family violence in CALD communities
People from CALD communities were identified by the RCFV as a priority group affected by family violence. The estimated prevalence of family violence in CALD communities, significant risk factors, and barriers to accessing services are summarised below.
Prevalence
The RCFV highlighted that data about the prevalence of family violence in CALD communities is limited, mainly because there is no reliable data that paints a clear picture of the scale of the problem.290 Although some survey data suggests that members of CALD communities are overrepresented as victims of family violence when compared with the general population, it is thought that barriers to access, communication and social participation are likely to significantly understate the problem.291 A summary report of case reviews completed by the Coroners Court of Victoria concerning family violence related homicides found that of 271 family violence homicides examined, 10% involved a person or persons from a CALD background.292 These numbers are suspected to be an under-representation as only cases where country of birth was recorded were included in the study.
Contributing circumstances and specific presentations of family violence risk
People from CALD communities may experience a range of abuses which reflect unique presentations of evidence-based family violence risk factors. Presentations of family violence that disproportionately affect people from CALD communities include:
- Social isolation: People from CALD backgrounds are at a higher risk of social isolation dueto language barriers, having fewer contacts within the community and living far away from theirfamily. Perpetrators of abuse may exploit this by preventing the person from learning Englishor having contact with people outside of the family unit, exacerbating social isolation. Victims also risk being ostracised by the community and their family if they speak up or leave an abusive relationship.293
- Forced marriage: Forced marriage refers to a marriage which takes place without free and full consent from one or both parties. Forced marriages are distinct from arranged marriages, which involve a marriage organised by families but where the individuals involved have the right to accept or reject the marriage. Forced marriages may involve the union between individuals who are children and not capable of providing free and full consent. As highlighted by the RCFV, “forced marriages can represent an intersection between family violence, sexual exploitation and child protection”.294
- Female genital mutilation: Female genital mutilation, female cutting or female circumcision refers to any procedure involving the total or partial removal of female genital organs for nonmedical purposes. The practice has been documented to take place in Africa, Asia and the Middle East, and is propagated for a variety of cultural reasons. Female genital mutilation is a crime in Australia. It is also generally viewed as a form of family violence as it is a means of controlling women and girls. The practice is known to be harmful and has both immediate and long-term health impacts.295
- Financial abuse: While financial abuse is not unique to CALD communities, it is recognised as being a particular concern for these groups. Coupled with the social isolation that people in CALD communities often experience, victims may become entrenched in an environment where financial abuse is more likely to occur and impact a person’s ability to support themselves. Financial abuse can include one party controlling all household finances, refusing access to bank accounts or services (such as having a phone plan) or forcing a party to work without payment or access to earnings.
- Dowry-related violence: A dowry is a monetary or physical gift transferred from a bride’s family to her husband’s after marriage. Marriages involving dowries are most common in Indian, Pakistani, Sri Lankan, African and Middle Eastern communities. Dowry-related violence may occur following claims that a dowry was not paid or from coercive demands for additional money or gifts. In some cases, men may use immigration-related threats to try leverage a higher dowry. Women who have tried to report abuse stemming from dowries have faced additional barriers from the criminal justice system, with some women having found that police do not understand what they are talking about when discussing dowries.296
- Spiritual abuse: While spiritual abuse is not unique to CALD communities, in some instances, perpetrators of family violence use faith to condone or excuse their behaviour. This is described as spiritual abuse, which is “the use of religion to justify gender inequality and to justify violence against women”.297
- Multi-perpetrator violence: The involvement of multiple perpetrators in family violence is reported to be more common within CALD communities. This occurs when multiple family members, extended family or social networks are involved in controlling the victim’s behaviour.298
- Immigration-related abuse: This abuse can involve deliberately providing misinformation about a person’s visa status, hiding passport or immigration documents, and threatening deportation. These are some of the control tactics used by perpetrators of family violence against refugees and immigrants from CALD backgrounds. In these instances, perpetrators capitalise on the victim’s uncertainty about their rights and entitlements in order to continue the violence.299
Family violence in CALD communities can also be exacerbated by characteristics or circumstances that can be more common in those communities, including:
- Pre-arrival trauma: It was noted by the RCFV that traumatic experiences prior to arrival in Australia can increase the incidence of family violence. It is acknowledged that some people from CALD backgrounds have come to Australia to escape war and persecution in their home countries. Frustration, anxiety and anger associated with this trauma may manifest into violence directed towards family members.300
- Immigration status: CALD victims who do not have permanent residency and depend on their partner for their visa status are particularly vulnerable to family violence. Often, they are not eligible for services such as Medicare, and they could be deported or lose custody of their children if they leave the relationship. Knowledge of the potential ramifications for a person’s visa status could be used by an abusive partner to threaten and control the victim, thus creating a power imbalance.301
- Different cultural understandings of what constitutes family violence: CALD victims may lack an understanding of what constitutes family violence; particularly if they are from countries or cultures where family violence is not viewed as a crime or where it can be considered the norm for men to ‘discipline’ their female partner due to gender inequality.302 In their submission to the RCFV, the Victorian Foundation for Survivors of Torture (Foundation House) noted that some people living in Australia come from countries and cultures where violence within a family is acceptable.303 Foundation House highlighted that due to a lack of understanding of the Australian legal system, both men and women may not know that family violence is prohibited and stretches beyond physical violence to emotional, psychological and financial abuse.304 This can result in people from CALD communities not identifying themselves as victims of family violence or being unsure how to report and seek assistance
- Difficulties leaving a violent relationship: CALD people may be reliant on their partner for money, transport and language,305 which limits their ability to leave an abusive relationship. A lack of culturally appropriate crisis accommodation may also increase the difficulty people from CALD backgrounds face when attempting to escape family violence.306
Under-reporting and barriers to accessing services
The RCFV highlighted that people from CALD communities are generally less likely than members of other community groups to speak out or report family violence. This may happen for a number of
reasons, including but not limited to:307
- a perception that services will not provide a culturally sensitive response
- language barriers
- social isolation
- shame and stigma involving others in family matters
- fear of being ostracised from their community
- fear and mistrust of government agencies
- cultural norms that set out gender roles, sexuality, marriage, divorce and family dynamics
- lack of CALD specific support services
- a lack of available and independent interpreters.
The RCFV outlined in detail the reluctance that people from CALD communities have when disclosing family violence to government, law enforcement and even people outside of the family unit.
Why do we need to collect CALD information?
The consistent collection of cultural and linguistic diversity information from people coming into contact with the family violence system is vital for a number of reasons. Firstly, anecdotal evidence and research surrounding family violence and people from CALD communities in Australia indicates that this group should be considered as a priority in future responses to family violence, due in part to the unique barriers these communities face when trying to report abuse and access services. Additionally, CALD information is necessary for operational reasons. Collecting information about a person’s primary language and whether they need an interpreter, for instance, often satisfies an operational requirement when providing a service. Finally, there are gaps in our present understanding of how family violence impacts people from CALD communities. In particular, there is limited evidence collected in surveys and administrative data which can be used to make informed decisions about service use, intervention strategies and risk assessment targeting family violence in CALD communities. In order to better understand the range and impact of family violence in these communities, effort needs to be directed at improving the consistency and comparability of data collection practices within Victoria.
Operational need to collect
In Victoria, the government and its funded agencies have a duty of care to ensure that members of the public understand the information that is being provided to them. This duty of care may be breached if a service or agency unreasonably fails to provide or inform a client about their right to an interpreter.308 Therefore, it is an operational requirement in Victoria to determine whether an interpreter is required by a person accessing a government funded service. Record management systems should be able to accommodate the collection of this data item. If this information is collected consistently, it can better inform the demand for translation services and the types of languages required.
Gaps in information
As previously discussed, information pertaining to the nature and prevalence of family violence in CALD communities is limited due to a lack of understanding of family violence in CALD communities, fear of reporting and barriers to accessing services. The RCFV further noted that surveys in Australia are not specifically designed to capture information on experiences of family violence by people in CALD communities. It is speculated that the under-representation of people from CALD backgrounds in survey data may be related to people from these communities being less likely to engage with
surveys or discuss violence with a survey interviewer.309
Additionally, the collection of CALD information in Victoria is inconsistent and difficult to compare. Currently, most service providers and agencies collect some information about cultural and linguistic diversity, however, there is little parity between organisations regarding the data items that are collected. For instance, many services and agencies collect information about a person’s need for an interpreter, but it is often not comparable due to the use of different language classifications. Many agencies will collect other data items about CALD communities, but the particular data items often vary. The inconsistency and variety of information collected has limited use for further analysis and comparison.
Challenges in current data collection practices
There are number of challenges which can impact the ability to collect information on CALD communities. Challenges that are relevant to CALD communities include:
- Data collection is not core to business function, with the collection of the full range of CALD information therefore not seen as a priority
- Lack of training in collection of data that may be perceived as sensitive, which can lead to a reluctance from workers to collect information about a person’s cultural background for fear of impacting the client/worker relationship, or being discriminatory
- The requirement for multiple data items to fully record CALD identity can create challenges for IT systems that do not have the capacity to include detailed response options.
Of particular relevance is the impact of varied operational requirements and business requirements may result in data collection that is partial, or difficult to compare. For example, some organisations may need to collect information on a person’s visa status, for instance, in order to ascertain if an individual is eligible for a service, whereas other organisations may be obliged to collect information on a person’s requirement for an interpreter. As a result, the range of CALD data items and response options varies across agencies, which contributes to the accumulation of data which are not comparable between services.
Prior to implementing the proposed data collection standards, agencies should be aware of some of the challenges they may encounter in collecting data from CALD communities. Reference to these challenges is not intended to deter agencies from collecting CALD information, but rather to inform them in their preparation for data collection. Considerations for specific data items are discussed in the proposed data collection standard below.
Existing data standards
In Victoria, there is currently no consistent method of collecting CALD information and consequently, the data collected within the context of family violence are inconsistent across administrative data sources. The primary data standards that currently exist for the collection of CALD information were developed by the ABS. These standards include all data items that can be collected to identify a person’s cultural background and main languages spoken.
ABS Standards
The ABS have many data standards which capture different cultural and linguistic characteristics. When these standards are used together, they allow for a broader understanding of a person’s origin and cultural diversity. They include:
- country of birth standard,310 which includes the data items:
- country of birth of person
- country of birth of father
- country of birth of mother
- language standards,311 which include 5 data items:
- main language other than English spoken at home
- proficiency in spoken English
- first language spoken
- languages spoken at home
- main language spoken at home
- Indigenous status standard312
- ancestry standard313
- religious affiliation standard314
- year of arrival standard315
It should be noted that Indigenous status data collection is addressed in the section on Aboriginal and Torres Strait Islander communities. Combinations of these data standards are used across government to collect CALD information. In the context of administrative data, questions from these data standards are often combined with questions required for operational purposes, such as the requirement for an interpreter.
Data collection standard for collecting information from CALD communities
There is no single data item that can capture a person’s cultural background and it is therefore advised that a number of data items are used to identify the different facets of a person’s cultural identity. The purpose of this data collection standard is to provide a set of questions that can be asked of a client in a service provision context, which are collected as part of an administrative dataset. Through research and consultation, the following four data items have been deemed most relevant in collecting CALD information and practical for service providers to ask:
- country of birth
- cultural background and ethnicity
- main language spoken at home
- interpreter required
The four data items included in this standard have been chosen for their value in providing useful information about a person’s cultural and linguistic diversity. However, this does not negate the need for ongoing, qualitative consultation with CALD communities to ensure the data items remain current with community standards and adapt to shifts in modes of identification. It may therefore be necessary to revise the standard if other data items become more appropriate and relevant in the future.
For each of these data items, an example short list has been used to demonstrate the application of the question. Please note that it is not recommended that short lists are used in actual data collection practice, as they cannot capture all possible responses. Instead, it is recommended that service providers and agencies use the full suite of response options included in the relevant ABS Standard classification. Links to these classifications have been included below each data item.
Before collecting CALD information, the purpose of data collection needs to be made clear to the client, and if applicable, linked to either a direct service response or referral to an appropriate service. There are also privacy implications related to the collection of some CALD information due to its sensitive nature. Relevant privacy legislation such as the Health Records Act 2001 (Vic) and the Privacy and Data Protection Act 2014 (Vic) should be considered by data custodians when collecting and storing this information. Further information about privacy and security considerations is provided on page 18.
Country of birth
Definition
Country of birth is defined as the country in which a person was born. This is an objective measure of whether a person was born in Australia or overseas and is just one component of understanding a person’s cultural background.
Question phrasing and response categories
|
In which country were you born? Note: The example option list presented below is based on the response categories used in the ABS country of birth standard. □ Australia |
Standard answer categories
The national ABS classification for country of birth is the Standard Australian Classification of Countries (SACC) 2016 (Cat. No. 1269.0).316 Where IT infrastructure permits, all countries in the classification should be available as responses, in order to remove the need for only a subset of countries to be shown and an ‘other’ response category. However, it is acknowledged that this may not be possible, and as such, a short list of countries can be created based on the agency’s requirements. Only one response category should be recorded for this data item.
Benefit of asking country of birth
Country of birth is a static and reliable data item that provides fundamental and objective information about a person’s origins. Country of birth forms part of the current data collection practices of many agencies and is also collected in the Census of Population and Housing, enabling comparison and analysis with existing Census data. When collected in conjunction with the cultural background and ethnicity data item, it can be used as an indicator of the ethnic and cultural composition of a population.
Considerations in asking about country of birth
It should be noted that there are some sensitivities in asking a person their country of birth and that people may be hesitant or fearful to disclose this information if they believe it may negatively affect them in some way. It is recommended that each person is given the option to not disclose their country of birth in the form of the ‘prefer not to say’ response.
Cultural background and ethnicity
Definition
For the purposes of this framework, the terms ‘cultural background’ and ‘ethnicity’ can be used interchangeably. In the ABS Australian Standard Classification of Cultural and Ethnic Groups (ASCCEG) 2016 (Cat. No. 1249.0),317 ethnicity is defined as the shared identity or similarity of a group of people on the basis of one or more factors.318 These factors can include, but are not limited to:319
- a long shared history, the memory of which is kept alive
- a cultural tradition, including family and social customs, sometimes religiously based
- a common geographic origin
- a common language (but not necessarily limited to that group)
- a common literature (written or oral)
- a common religion
- being a minority (often with a sense of being oppressed)
- being racially conspicuous
This data item is designed to allow a respondent to self-identify with the culture or ethnicity that they most associate with.
Question phrasing and response categories
|
What cultural background or ethnicity do you identify with? Note. The example option list presented below contains the top 10 ancestries identified by people living in Victoria for the 2016 Census. □ None |
Standard answer categories
The national ABS classification for grouping ethnicity is the ASCCEG which is designed to be used for the classification of information relating to topics such as ancestry, ethnic identity and cultural diversity. The ASCCEG is a three-tier classification, allowing for the respondent to identify with a specific ethnicity that can then be aggregated into a broader cultural group.
Where IT infrastructure permits, all ethnicities in the ASCCEG should be available as responses, in order to remove the need for only a subset of ethnicities to be shown and an ‘other’ response category. However, it is acknowledged that this may not be possible, and as such, a short list of ethnicities can be created based on the agency’s requirements. Additionally, where possible, multiple responses should be accepted for this data item in order for a respondent to list all ethnicities and cultures that they identify with.
Benefit of asking cultural background and ethnicity
There is an increasing movement towards asking people about the cultural background or ethnicity they most closely identify with. This is not necessarily based on their birthplace but a combination of the culture and ethnic group that they feel aligned with. Given the long history of world migration, it has become increasingly common for a person to be born in one country but identify strongly with the culture of another country.
Considerations in asking cultural background and ethnicity
There are a number of considerations that should be taken into account when asking about a person’s cultural background or ethnicity. As a person’s ethnicity is self-identified, a person should be able to disclose any ethnicity regardless of their country of birth. The cultural background or ethnicity that a person identifies with can change over time, and as such, it should be possible to update a person’s response to this question and maintain a historical record of changes where IT infrastructure allows.
It should also be noted that there are some sensitivities in asking this question and that people may be hesitant or fearful to disclose their cultural background if they believe it may negatively affect them in some way. It is recommended that each person is given the option to not disclose their cultural background and ethnicity in the form of the ‘prefer not to say’ response.
Main language spoken at home
Definition
Main language spoken at home is the main language spoken by a person in the home on a regular basis to communicate with other residents and regular visitors to the home.320
Question phrasing and response categories
|
Which language do you mainly speak at home? (If more than one language, indicate the one that is spoken most often.) Note. The example option list presented below is based on the response categories used in the ABS Languages standard. □ English |
Standard answer categories
The ABS national classification for grouping languages is the Australian Standard Classification of Languages (ASCL) 2016 (Cat. No. 1267.0).321 This classification is designed to be used for the classification of a number of language variables including first language spoken, languages spoken at home, main language spoken and main language other than English spoken at home. The ASCL recognises that some people use non-verbal forms of communication and therefore includes Auslan and other sign languages as response options. While the ASCL includes dialects, it may not be an exhaustive list, and agencies may therefore need to use the free text field to record the dialect spoken.
Where IT infrastructure permits, all languages in the classification should be available as responses, in order to remove the need for only a subset of languages to be shown and an ‘other’ response category. However, it is acknowledged that this may not be possible, and as such a short list of languages can be created based on the agency’s requirements. As this data item pertains to the main language spoken at home, only one response category should be recorded for this data item, which is in line with the ABS Standard.
Benefit of asking main language spoken at home
The ABS Language Standards 2016 currently contain five language data items. However, main language spoken at home has been included in this data collection standard as it was identified through research and consultation as the most useful general purpose language variable. It indicates the language a person is likely to be most comfortable using, and can also be used to gauge the English proficiency of the household.
Considerations in asking main language spoken at home
As with the other data items relating to cultural and linguistic diversity, there may be similar sensitivities in asking this question. A ‘prefer not to say’ option should be included to allow people not to disclose this information.
Interpreter required
Definition
The interpreter required data item assesses a person’s need for an interpreter as perceived by the person or someone consenting for the person. This is an operational question that should be asked by service providers and agencies who need to verbally communicate with a person.
Question phrasing and response categories
|
Do you require an interpreter? Note. The example option list presented below is based on the response categories used in the ABS Languages standard. □ No (skip next question) Which language do you require? □ Mandarin For office purposes only: which language was provided? __________________________ |
Standard answer categories
To ensure consistency of data collection, agencies should collect the language information related to interpreter requirements consistent with the classification used when collecting a person’s main language spoken at home.
Where IT infrastructure permits, all languages from the ASCL should be available as responses, in order to remove the need for only a subset of languages to be shown and an ‘other’ category. However, it is noted that this may not be possible, and as such the above list should be amended to reflect the languages that are most frequently reported to the agency or service provider. Where a subset of languages is used it is important to use the same categories for both the ‘interpreter required’ and ‘main language spoken at home’ data items.
Office purposes only: Provision of interpreter and language spoken
This additional question, designed for use by the service provider or agency, is intended to develop an understanding between the demand for interpreters with specific language skills and the availability of those interpreters. Research and consultation highlighted that it is commonplace for a person to request an interpreter to interpret a particular language, but due to a lack of interpreters they may be provided with an alternative interpreter, and must speak in a language that is not their preferred. In instances where an interpreter is not provided at all, ‘English’ should be recorded as the language provided. By collecting information on the language provided to the client, departments and agencies can better understand the gap between the demand for interpreters and the available supply.
Benefit of asking whether an interpreter is required
The consistent collection of this data item provides information about the languages spoken by the client base, and can be used to inform decisions about translation service that need to be provided in the future. In many service delivery settings it is a legal requirement that this information is recorded.
Considerations in providing interpreters
Organisations should be aware of the risk in small and emerging communities that the interpreter may know both parties involved in a family violence incident. In these cases, it may be beneficial to use another interpreter in a language nominated by the client.
The Victorian Government is updating its guidelines on the use of interpreters to deal with family violence (recommendation 157). This specifically relates to eliminating the use of perpetrators, children and other family members as interpreters, as well as the use of the same interpreter for both parties.322 Similarly, Victoria Police has amended the Code of Practice for the Investigation of Family Violence to highlight the risk of using the same interpreter for both parties as well as using children as interpreters, and training is being administered on the use of interpreters through Foundation Training programs and through the Centre of Learning for Family Violence (recommendation 159).323
The Department of Health and Human Services has produced guidelines for organisations working with interpreting and translating services. These include information on choosing the mode of interpreting (onsite, telephone or video remote), accommodating requests for a preferred interpreter or interpreter of a particular gender, and working with Auslan interpreters. For details of these guidelines, please refer to ‘Training and resources’ at the end of this section.
How to determine response categories
Across each of the classifications recommended in this data collection standard, there are many response values that can be provided by a respondent. Ideally, systems would allow for the selection of all of the response options which are listed in the SACC, ASCCEG and ASCL. The complete list of response options for all of these measures can be found in ‘Training and resources’ at the end of this section.
It is noted that IT infrastructure restrictions may not allow for an extensive list of response options to be utilised. In these instances, a short-list can be developed with an ‘other’ or an ‘other (please specify)’ free-text option. However, free-text methods are not the preferred option for ensuring quality data, particularly if there is no resourcing to code or clean these data fields.
If a short list of response categories is developed, it is important to note that if these categories are changed over time to align with the most common response categories, time series analysis may be restricted.
Why is this combination of data items important?
As mentioned earlier, there is no single data item that can be used to capture all people from CALD communities. Without asking questions relating to a person’s cultural background or ethnicity and main language spoken at home, it is not possible to capture important CALD information about a person. In only asking a person’s country of birth there is a risk that differences within communities such as cultural background are masked.324 While working with clients from CALD communities, it is important to understand each of these aspects of a person’s diversity to ensure that the service response and referral pathways are culturally sensitive and relevant to a person’s needs.
The following examples highlight the complexity of CALD information captured when using all four data items.
- Example 1. A person who was born in Australia but identifies their cultural background as Vietnamese and primarily speaks Vietnamese at home but does not require an interpreter.
- Example 2. A refugee who was born in Kenya but identifies ethnically as South Sudanese and requires an interpreter because they primarily speak Dinka and have limited English.
- Example 3. A person who was born in Malaysia but identifies their ethnicity as Malaysian Chinese and requires an interpreter because they primarily speak Mandarin and have limited English.
- Example 4. A person who was born in India but identifies as British and doesn’t require an interpreter as they do not speak any language other than English at home.
Other data items considered
The following data items were considered in the development of this framework but were not included in the final set of data items for this data collection standard. The benefits of each are outlined below, along with rationale on why they were not included. Some services and agencies may already collect these data items. In these circumstances, it is recommended that organisations continue to collect all data items essential for operational purposes, in addition to the four data items included in the proposed standard above. In general, the collection of these data items by other services and agencies is encouraged where it is feasible, appropriate and complies with privacy legislation.
English proficiency
English proficiency is a subjective measure of a person’s competence in spoken English, which may be used as an indication of a person’s level of integration into society, and how much assistance they will require navigating services. This data item should follow another question about language which filters out people whose only language is English, as it is intended to assess the ability of people who speak languages other than English. It was determined that when the interpreter required data item is recorded, the use of English proficiency is a duplication, in that it is another way to determine a person’s ability to communicate effectively with the system and understand the process and their rights.
Visa status/migration status
Throughout consultation, visa and migration status were discussed as valuable pieces of information to understand whether a person is entitled to certain social services and assistance, such as an immigration lawyer. Visa status may also be used by a person as a means of exerting control over another person in a family violence situation, and may therefore be useful to capture in a family violence service context to determine a person’s vulnerability. It is strongly recommended that agencies collecting this data item carefully explain the reasons for doing so, and inform the person that the information will not be used against them. Additionally, staff would require training in how to accurately record the complexity of visa categories. Visa status was excluded from this data collection standard as it has the potential to deter people from disclosing or reporting family violence if they fear they will lose their right to stay in Australia. However, this information can be asked if it is required for agencies and service providers to perform operational functions.
Year of arrival in Australia
As with visa/migration status, the year of arrival variable was extensively discussed during consultation. It was identified that new and emerging communities face more challenges than established migrant communities when settling in Australia, due to the need for interpreters and a lack of extended family and social networks. Year of arrival in Australia may indicate the person’s familiarity with Australian society and laws, level of exposure to and awareness of information and service systems, and degree of social connectedness. When collecting this data item, it is important that country of birth is asked first, as agencies should only ask for year of arrival if a person was born outside of Australia. Agencies should also be mindful that this variable measures the year of first arrival in Australia and not the year of most recent arrival. Significant periods spent outside of Australia need to be accounted for when making determinations about the person’s period of residence in Australia. Ultimately, the year of arrival variable was not included in this data collection standard as it was not deemed to be as high priority as some of the other data items, which provide more detailed information about a person’s background and potential needs.
Religious affiliation
During consultations, it was noted that asking a person to identify the religious beliefs they adhere to or religious group to which they belong can assist agencies in providing more culturally appropriate services. For example, people of certain faiths may prefer to be assigned a case worker of a particular gender. In this instance, the collection of religious affiliation allows for better allocation of culturally appropriate case workers. It is also important to recognise that people born in the same country may have had vastly different life experiences as a result of their faith, which also means that they are likely to encounter different barriers when attempting to seek help for family violence. Collection of religious affiliation therefore provides meaningful information about a person’s background that can be used to tailor service responses. However, agencies need to consider whether asking for religious affiliation is appropriate within the context of the service they are providing. There are particular sensitivities in asking this question and people may be hesitant to disclose this information due to persecution in their country of origin or fear of negative consequences.
Ancestry
Asking about a person’s ancestry provides information about their origins and heritage. When used in combination with other variables, it can measure the extent to which people retain the ethnicity and culture of their ancestors. It was discussed as an alternative to cultural background and ethnicity, but given it is based on the origins of a person’s mother, father and earlier generations, it does not necessarily reflect a person’s own affiliation or alignment with a particular country, culture or faith. As such, cultural background and ethnicity was chosen to support the movement towards allowing people to self-identify their own culture.
Country of birth of father/mother
Collecting the country in which a person’s parents were born can be used to better understand a person’s cultural background and determine retention of culture, ethnicity and language. Throughout consultation, data items which captured details about the person were deemed more relevant and preferred to data items which captured details about a person’s father/mother.
Main language other than English spoken at home
Asking for the main language other than English spoken at home is particularly beneficial for established migrant communities that may have developed proficiency in English, but still use another language at home. It is used in the Census, which allows for the comparison of administrative data with Census data for analysis. Main language spoken at home was chosen in preference to this data item for its ability to better gauge English proficiency.
Training and resources
Australian Standard Classification of Cultural and Ethnic Groups (ASCCEG)
Outlines the full list of response options for the cultural background and ethnicity data item.
Website: www.abs.gov.au/ausstats/abs@.nsf/mf/1249.0
Australian Standard Classification of Languages (ASCL)
Outlines the full list of response options for the main language spoken at home and interpreter required data items.
Website: www.abs.gov.au/ausstats/abs@.nsf/mf/1267.0
Ethnic Communities Council of Victoria
Advocates on behalf of multicultural communities in a range of different areas.
Website: www.eccv.org.au
Phone: 03 9354 9555
How to work with interpreters and translators: A guide to effectively using language services
Guidelines designed by the Department of Health and Human Services to assist organisations in providing language services to clients and responding to the needs of Victoria’s diverse community.
Website: dhhs.vic.gov.au/publications/language-services-policy-and-guidelines
inTouch – Multicultural Centre against Family Violence
Provides services, programs and responses to issues of family violence in migrant and refugee communities.
Website: www.intouch.org.au
Phone: 03 9413 6500
Standard Australian Classification of Countries (SACC)
Outlines the full list of response options for the country of birth data item.
Website: www.abs.gov.au/ausstats/abs@.nsf/mf/1269.0
Translating and Interpreting Service
National interpreting service operated by the Department of Home Affairs, which is available to government agencies and businesses 24 hours a day, seven days a week. They provide immediate and pre-booked phone interpreting, as well as onsite interpreting services.
Website: www.tisnational.gov.au
Phone: 131 450
Victorian Multicultural Commission
Provides independent advice to government to inform the development of policies and services to culturally, linguistically and religiously diverse communities. A comprehensive directory of useful resources can be accessed from their website.
Website: www.multicultural.vic.gov.au
Phone: 03 7017 817
VITS LanguageLoop – Victorian Interpreting and Translating Service
Provides professional interpreting and translating services to government agencies and businesses 24 hours a day, seven days a week. Their services include document translation, telephone translation and onsite interpretation.
Website: www.languageloop.com.au
Phone: 03 9280 1941
285 RCFV 2016, Volume 5 Report and recommendations, p.99.
286 Ethnic Communities Council of Victoria 2012, ECCV Glossary of Terms, viewed 21 June 2018, www.eccv.org.au/library/file/document/ECCV_Glossary_of_Terms_23_October.docx
287 Ibid.
288 ABS 2013, 3417.0 Understanding Migrant Outcomes – Enhancing the Value of Census Data, Australia 2011, viewed 21 June 2018, www.abs.gov.au/ausstats/abs@.nsf/mf/3417.0
289 RCFV 2016, Volume 5 Report and recommendations, p.99.
290 Ibid p.101.
291 Ibid.
292 Walsh, C, McIntyre, S-J, Brodie, L, Bugeja, L & Hauge, S 2012, Victorian Systemic Review of Family Violence Deaths – First Report,
Coroners Court of Victoria, Melbourne, p.22.
293 RCFV 2016, Volume 5 Report and recommendations, p.105.
294 Ibid p.111.
295 Ibid.
296 Ibid p.122.
297 Ibid p.136.
298 Vaughan, C, Davis, E, Murdolo, A, Chen, J, Murray, L, Quiazon, R, Block, K & Warr, D 2016, Promoting community-led responses to violence against immigrant and refugee women in metropolitan and regional Australia [Research Report], Australia’s National Research Organisation for Women’s Safety, Sydney.
299 Ibid.
300 RCFV 2016, Volume 5 Report and recommendations, p.109.
301 Ibid.
302 Ibid p.108.
303 The Victorian Foundation for Survivors of Torture (Foundation House) 2015, Submission to the Royal Commission into Family
Violence, no. 925, viewed 22 June 2018, www.rcfv.com.au/Submission-Review
304 Ibid.
305 RCFV 2016, Volume 5 Report and recommendations, p.105.
306 Ibid p.108.
307 Ibid p.106.
308 Victorian Multicultural Commission, Using interpreting services, viewed 22 June 2018, www.multicultural.vic.gov.au/projects-andinitiatives2/improving-language-services/standards-and-guidelines/using-interpreting-services/using-interpreting-services-page-2#duty-ofcare
309 RCFV 2016, Volume 5 Report and recommendations, p.101.
310 ABS 2016, 1200.0.55.004 Country of Birth Standard, 20 16, viewed 22 June 2018, www.abs.gov.au/ausstats/abs@.nsf/mf/1200.0.55.004
311 ABS 2016, 1200.0.55.005 Language Standards, 2016, viewed 22 June 2018, www.abs.gov.au/ausstats/abs@.nsf/mf/1200.0.55.005
312 ABS 2014, 1200.0.55.008 Indigenous Status Standard, 2014, version 1.5, viewed 22 June 2018, www.abs.gov.au/ausstats/abs@.nsf/mf/1200.0.55.008
313 ABS 2014, 1200.0.55.009 Ancestry Standard, 2014, Version 2.1, viewed 22 June 2018, www.abs.gov.au/ausstats/abs@.nsf/mf/1200.0.55.009
314 ABS 2016, 1200.0.55.003 Religious Affiliation Standard, 2016, viewed 22 June 2018, www.abs.gov.au/ausstats/abs@.nsf/mf/1200.0.55.003
315 ABS 2014, 1200.0.55.007 Year of Arrival Standard, 2014, viewed 22 June 2018, www.abs.gov.au/ausstats/abs@.nsf/mf/1200.0.55.007
316 The full classification of countries can be found at www.abs.gov.au/ausstats/abs@.nsf/cat/1269.0
317 The full classification of cultural and ethnic groups can be found at www.abs.gov.au/ausstats/abs@.nsf/cat/1249.0
318 ABS 2016, 1249.0 Australian Standard Classification of Cultural and Ethnic Groups (ASCCEG), 2016, viewed 22 June 2018,
www.abs.gov.au/ausstats/abs@.nsf/mf/1249.0
319 Ibid.
320 ABS 2016, 1200.0.55.005 Language Standards, 2016, viewed 22 June 2018, www.abs.gov.au/ausstats/abs@.nsf/mf/1200.0.55.005
321 The full classification of languages can be found at www.abs.gov.au/AUSSTATS/abs@.nsf/mf/1267.0
322 RCFV 2016, Volume 5 Report and recommendations, p.123.
323 State Government of Victoria, Victoria Police amend the Code of Practice around the use of interpreters, viewed 22 June 2018, https://www.vic.gov.au/family-violence-recommendations
Data collection standards - Aboriginal and Torres Strait Islander communities
Outlines some of the family violence issues faced by Aboriginal people, challenges in collecting data, information gaps, and the existing national standard for the collection of Indigenous status.
In their report and recommendations, the RCFV noted that Aboriginal and Torres Strait Islander people disproportionately experience family violence, and face unique barriers to accessing assistance.325 The RCFV has detailed the issues and injustices experienced by Aboriginal people that have had a profound and lasting effect.
Dhelk Dja: Safe our way – Strong Culture, Strong Peoples, Strong Families (Dhelk Dja Agreement) defines family violence in the context of Aboriginal communities as ‘an issue focused around a wide range of physical, emotional, sexual, social, spiritual, cultural, psychological and economic abuses that occur within families, intimate relationships, extended families, kinship networks and communities. It extends to one-on-one fighting, abuse of Indigenous community workers as well as self-harm, injury and suicide.’ The Dhelk Dja Agreement’s definition of family violence also acknowledges the impact of violence by non-Aboriginal people against Aboriginal partners, children, young people and extended family on spiritual and cultural rights, which presents as exclusion or isolation from Aboriginal culture and/or community. The Dhelk Dja Agreement’s definition includes elder abuse and the use of lateral violence within Aboriginal communities. It also emphasises the impact of family violence on children and young people.326
The findings of the RCFV highlighted that while data currently available indicates an overrepresentation of Aboriginal people affected by family violence, there are considerable inadequacies in the collection of data concerning Aboriginal people across agencies and departments. This hinders our full understanding of the extent of family violence experienced by Aboriginal people.
One of the RCFV recommendations focussed on the “[improvement of] the collection of Indigenous specific data relating to family violence”.327 In addressing this recommendation, this section of the framework will outline some of the family violence issues faced by Aboriginal people, challenges in collecting data, information gaps, and the existing national standard for the collection of Indigenous status. Finally, a number of recommendations have been made to assist agencies in the collection of data concerning Indigenous status and interim solutions that can be used to improve analysis and reporting of the data currently available.
Terminology and definitions
Nationally, the term ‘Indigenous’ has been used to describe Aboriginal and Torres Strait Islander people across all state and territory jurisdictions. Therefore, the nationally endorsed question used to determine whether a person is Aboriginal and/or Torres Strait Islander is called the Standard Indigenous Question (SIQ), and the collected variable is often referred to as ‘Indigenous status’. As noted by the ABS, the term ‘Indigenous’ is not a specific descriptor and some Aboriginal people feel the term diminishes their identity or fails to recognise the cultural diversity that exists within the collective population.328 For the purposes of this section, the term ‘Indigenous’ is used only when referring to the collected variable ‘Indigenous status’. Otherwise, the term ‘Aboriginal’ is used, and this refers to both Aboriginal and Torres Strait Islander people.
Family violence and Aboriginal communities
The RCFV identified people from Aboriginal communities to be a priority when considering service response to family violence events, due in part to the prevalence of family violence affecting Aboriginal people, the types of family violence experienced, and the profound impact that colonisation has had on the psychological, social and economic outcomes for people in these communities.
Family violence is not part of Aboriginal culture, and Aboriginal cultural ways are based on strong families and kinship systems. As noted by Djirra (formerly the Aboriginal Family Violence Prevention and Legal Service Victoria or ‘FVPLS Victoria’) in their submission to the RCFV, “there are multiple complex and diverse factors contributing to the high levels and severity of family violence in Aboriginal and Torres Strait Islander communities, and it must be clearly understood that the causes do not derive from Aboriginal culture”.329 Additionally, it is important to highlight that not all perpetrators of family violence towards Aboriginal people are Aboriginal themselves. In their submission to the RCFV, Djirra stated that it routinely sees clients, mostly women, who experience family violence at the hands of men from a range of different backgrounds and cultures, both Aboriginal and non-Aboriginal.330
Prevalence
Despite gaps in data collected on family violence in Aboriginal communities, the information that is available clearly identifies an over-representation of Aboriginal women and children who are affected by family violence. Based on the 2014-15 National Aboriginal and Torres Strait Islander Social Survey (NATSISS), approximately 2 in 3 Aboriginal women (63%) and 1 in 3 Aboriginal men (35%) who had experienced physical violence in the previous year, reported that the perpetrator of the most recent incident was a family member, including a current or previous partner.331
The RCFV highlighted in their report that Aboriginal women and children experience greater family violence than other members of the community. Regardless of where they live, Aboriginal women are one of the groups at highest risk of family violence in Victoria.332 It has been estimated that Victorian Aboriginal women are 45 times more likely to experience family violence than non-Aboriginal women.333 When giving evidence to the RCFV, Antoinette Braybrook, the Chief Executive Officer of Djirra, stated that although they provide services to all Aboriginal victims, 93 percent of their clients are women.334
The link between family violence and child removal was consistently identified in RCFV submissions, consultations and evidence as an area where urgent attention is required,335 and research has found that men’s violence against women is a primary driver in up to 95% of Aboriginal children entering out-of-home care.336
In their 2018 report ‘Family, domestic and sexual violence in Australia’, the AIHW highlighted the high prevalence of family violence experienced by Aboriginal people, and noted that:337
- Two in five Aboriginal homicide victims were killed by a current or former partner, compared with one in five non-Aboriginal homicide victims.
- Aboriginal women were 32 times, and Aboriginal men 23 times, as likely to be hospitalised due to family violence as non-Aboriginal women and men.
Contributing circumstances and specific presentations of family violence risk
There are a number of overlapping circumstances which may contribute to and shape the experience of family violence for people from Aboriginal communities. Many of these factors may stem from the current and historical impact of colonisation and systemic discrimination against Aboriginal people.
The RCFV noted that one of the 11 guiding principles set out in the Victorian Indigenous Family Violence Task Force report is the recognition that “from an Indigenous perspective the causes of family violence are located in the history and impacts of white settlement and the structural violence of race relations since then”.338 The RCFV further detailed findings from consultations, submissions and evidence which noted the effect that white settlement, the Stolen Generations, and the devastation of Aboriginal cultures have had on Victorian Aboriginal communities.339 It is therefore important to examine family violence as it affects Aboriginal people within the context of the lasting impact of colonisation, and dispossession of land and culture.
This includes consideration of:340
- inter-generational trauma
- dispossession of land
- forced removal of children
- interrupted cultural practices that mitigate against interpersonal violence
- disproportionate rates of criminalisation and incarceration
- economic exclusion and poverty
- systemic and indirect racism
In their 2018 report, the AIHW noted that in addition to experiencing overall higher rates of family violence, Aboriginal people may be subjected to higher rates of physical violence and sexual abuse.
According to the 201415 NATSISS, 22% of Aboriginal Australians aged 15 and older reported experiencing physical or threatened physical violence.341 In addition, based on the ABS 2016 recorded crime data, Aboriginal Australians were up to 3.4 times as likely to be the victim of sexual assault as non-Aboriginal Australians.342 The AIHW report also highlighted that Aboriginal people were more likely to experience image-based abuse, which occurs when intimate or sexual photos or videos are shared online without consent.343
Under-reporting and barriers to accessing services
Aboriginal people face a wide array of complex and compounding barriers to reporting family violence and accessing support services.344 These include a fear of the consequences of reporting, lack of access to support services, mistrust of government and the legal system, and discrimination and racism.345 In some rural areas, people may not be able to find nearby services. When Aboriginal people access mainstream services, they may encounter discrimination, and language and cultural barriers.346
The RCFV heard that high rates of child removal and child protection intervention deter some Aboriginal women from disclosing family violence or seeking assistance.347 They also heard that Aboriginal women’s fear of having their children removed was not sufficiently understood by child protection workers.348
Why do we need to collect Aboriginal information?
Without accurate and consistent collection of data on Aboriginal people, it is difficult to determine the prevalence of family violence in these communities. While the existing data reveals an overrepresentation of Aboriginal people in the family violence system, limited and inconsistent data collection means that this proportion may be even greater. It was noted during the RCFV that “the collection of data about Aboriginal family violence by agencies is generally poor”,349 and that there are gaps both in existing survey and administrative data which affect our current understanding of family violence experienced by Aboriginal people. Comparable collection and recording of Indigenous status in administrative data are essential for informing service demand and measuring service effectiveness, and reliable data are required for planning, developing policies and making improvements in service delivery.350 Examples of gaps in information which currently exist are noted below.
Gaps in information
The RCFV found that the lack of data collection regarding Indigenous status is a significant concern in relation to the flow-on effect for service provision. If Indigenous status is not collected in the context of a family violence incident, then this information will not be included in formal referrals. This means that existing mechanisms to notify ACCOs cannot be deployed.351
Often, Indigenous status is only collected from one member involved in or seeking a service regarding a family violence incident. Where possible and appropriate, Indigenous status should be collected from all parties involved. The RCFV heard that there were many instances where Aboriginal children were not identified as such.352 As noted previously in the ‘Children and young people’ section, details about children affected by family violence are either not collected, or exist in case notes and therefore cannot be suitably used for data analysis. This approach not only devalues the impact of family violence on a child, but it also compromises the quality of administrative data collected. If information about children is not collected, Aboriginal children and young people will continue to be underrecorded in administrative data.
Gaps in survey data
In Australia, there are a number of surveys which collect information on the health and welfare of Aboriginal people. Despite these efforts, information concerning family violence and Aboriginal people is limited as information collected often does not directly examine the occurrence of family violence. The ABS NATSISS collects detailed information on a range of social issues including self-assessed health, disability, social networks, physical violence and safety. However, the survey was not designed to specifically capture all types of family violence and as such, results cannot reliably inform about rates and types of family violence affecting Aboriginal people. By contrast, the ABS Personal Safety Survey (PSS) is a key measure in Australia which examines the prevalence of family, domestic and sexual violence in the general population. However, because of the small sample size of this survey, it does not collect many data items which identify specific communities, including Indigenous status. The ABS Crime Victimisation Survey (CVS) is a broader survey which collects information about people’s experiences of crime victimisation. While this survey does collect Indigenous status, information collected about family violence is limited to physical assault and threats.
Challenges in current data collection practices
Prior experiences of discrimination and racism may result in reluctance to identify as Aboriginal due to fear of negative consequences, particularly when it is unclear what the information will be used for and how it is pertinent to the delivery of a service.353 A review undertaken by the ABS in 2014 highlighted that many Aboriginal people did not understand why the question was being asked or what the response would be used for, which could lead to unwillingness to answer the question.354 Additionally, Aboriginal people may be reluctant to identify if they do not believe that an agency will provide culturally sensitive services or treatment.
Practice of referring clients to Aboriginal-specific services
An important aspect of self-determination is that Aboriginal people have the right to choose to receive services from ACCOs where they are available.355 However, it was noted by the RCFV that when Aboriginal people access non-community specific services, an assumption is sometimes made by a service that the person should use a community-specific service.356 Inability to access mainstream services can conjure feelings of rejection and discourage Aboriginal people from seeking assistance in the future.357 Agencies and service providers should therefore ensure that Aboriginal people are given a choice regarding whether they would prefer to receive service from an ACCO or a mainstream service, rather than make an assumption based on a person’s collected Indigenous status.
Broader definitions of family violence used by Aboriginal communities
In the Family Violence Protection Act 2008 (Vic) (FVPA), the term ‘family member’ is defined broadly to include intimate partners, relatives and ‘familial-like’ relationships. The FVPA states that “a relative for an Aboriginal or Torres Strait Islander person includes a person who, under Aboriginal or Torres Strait Islander tradition or contemporary social practice,358 is the person’s relative”. Aboriginal people may therefore view family violence as occurring between members of their larger family and kinship networks, including aunts, uncles, grandparents, cousins and others in the wider community, whereas non-Aboriginal people may view family violence less broadly.359 Extensive family kinship relationships in Aboriginal communities may make it difficult to distinguish between family and general violence, which in turn may affect the ability of non-community specific services to identify family violence for these communities.
Data collection standard for collecting information from Aboriginal communities
Indigenous Status Standard – Standard Indigenous Question (SIQ)
The framework recommends the use of the national Indigenous Status Standard, which was developed by the ABS. As previously noted, the nationally endorsed question in this ABS Standard is called the Standard Indigenous Question (SIQ), and the collected variable is often referred to as ‘Indigenous status’. The definition of Indigenous status in the ABS Standard is “whether or not a person identifies as being Aboriginal or Torres Strait Islander”.360 The SIQ is used in ABS data collections and has been adopted by other government agencies across Australia.361
A person’s Indigenous status is determined by their self-reported response to the ABS SIQ. Various articulations of the standard question can be found on the ABS website,362 and the standard question module is presented below.
Question phrasing and response categories
|
Are you of Aboriginal or Torres Strait Islander origin? (For persons of both Aboriginal and Torres Strait Islander origin, mark both ‘Yes’ boxes). □ No |
Standard answer categories
The response categories should not include abbreviations such as ‘ATSI’ and ‘TSI’ as these can be considered offensive. In addition, the terms ‘Aboriginal’ and ‘Torres Strait Islander’ must be capitalised. Although ‘prefer not to say’ is not actually included in the standard question module for the ABS SIQ, it is valid that a person may refuse to answer the SIQ, so a ‘prefer not to say’ option is recommended.
Where appropriate, agencies and service providers should consider asking a person whether they are of Aboriginal or Torres Strait Islander origin each time they come into contact with a service. It is reasonable to assume that a person’s willingness to self-identify as being of Aboriginal or Torres Strait Islander origin may change over time, and therefore, information should continue to be collected even if a person comes into repeat contact with a service, and should be stored appropriately so a history of responses can be kept. For more information about the development and application of the SIQ, please see the AIHWs paper on ‘National best practice guidelines for collecting Indigenous status in health datasets’.363
Considerations in asking the SIQ
It has been previously noted in the framework that ongoing organisational change and staff training relating to inclusive practice is vital, and that Aboriginal people have a right to culturally safe services. It is important to avoid making assumptions about how a person identifies, and staff need to be trained in how to sensitively and respectfully collect data from Aboriginal people. Many ACCOs are already working co-operatively with mainstream organisations on top of already significant demands.364 For information regarding organisations which offer Aboriginal cultural awareness and cultural safety training, please refer to ‘Training and resources’ at the end of this section.
| What is cultural safety? |
|---|
| A culturally safe environment is one where services are provided in a manner that is respectful of a person’s culture and beliefs, and that is free from discrimination. To ensure that an environment is culturally safe, mainstream service providers are required to analyse their organisational culture and ensure that it does not have a negative impact on the cultural rights of Aboriginal communities. This right is supported by Victorian and national legal instruments which uphold the rights of Aboriginal people.365 |
Aligning Aboriginal data collection to the SIQ
To ensure consistency and comparability across data sources, the best practice method for collecting Indigenous status data is to align to the national SIQ. In order to do this, an agency or service provider should take into account the following four elements.
(1) question phrasing and formatting
(2) response categories and formatting
(3) frequency of asking the question (for example, each time people come into contact with a service)
(4) the ability to account for people changing their response over time.
Where possible, efforts should be made to improve the collection of Indigenous status data to align with the national standard.
Training and resources
In order for organisations to be able to collect data from Aboriginal people in a respectful and sensitive way, organisations need to ensure that their policies and procedures are inclusive of Aboriginal people, and that staff are trained in practices that are culturally appropriate. The list of organisations below is not exhaustive, but seeks to provide some valuable resources for agencies and service providers in Victoria. Please note that many of the organisations listed have limited funding available for the services they provide. Thus, the training noted here may not be available on an ongoing basis. The information below is sourced from the websites of the organisations listed.
Training
Centre for Cultural Competence Australia
Provider of Australia’s only online accredited Aboriginal and Torres Strait Islander cultural competence course.
Website: www.ccca.com.au
Phone: 1300 240 944
Koorie Heritage Trust
Providers of half-day and full day face to face training in building Aboriginal cultural competency, including introductory training, and training in policy, partnership and leadership.
Website: www.koorieheritagetrust.com.au
Phone 03 8662 6300
Victorian Aboriginal Child Care Agency (VACCA)
VACCA’s Training and Development Unit offer a range of programs to organisations working in the field of child and family welfare, to strengthen relationships with Aboriginal organisations, families and communities. For more information about the external training workshops currently offered, see details below.
Website: www.vacca.org
Phone: 03 9287 8800
Email: trainingevents@vacca.org
Victorian Aboriginal Community Controlled Health Organisation Inc (VACCHO)
VACCHO’s Aboriginal cultural safety training builds on cultural awareness training and provides practical tips and skills that can be utilised to improve practice and behaviour, which assist in making Aboriginal people feel safe.
Website: www.vaccho.org.au/consultancy/cs
Cultural safety team: 03 9411 9411
Victorian Aboriginal Community Services Association Ltd (VACSAL)
Whilst VACSAL’s core business relates to advocacy and community service provision, an important part of VACSAL’s work relates to the design and delivery of cultural awareness programs. VACSAL have developed considerable expertise in the customisation and delivery of these programs.
Website: www.vacsal.org/programs
Phone: 03 9416 4266
Resources
Djirra (formerly the Aboriginal Family Violence Prevention and Legal Service Victoria)
Djirra’s Koori Women’s Place is located in Melbourne, and provides Aboriginal women with a place to connect with lawyers, join in cultural and social activities, and get personalised support from Aboriginal women who can accompany women to appointments, set up referrals and be trusted companions to women facing the challenges of family violence. Djirra offer a range of support services, as well as providing community education and early intervention and prevention programs.
Website: www.djirra.org.au
Phone: 03 9244 3333
Indigenous Status Standard
Detailed information regarding the ABS SIQ is available on the ABS website.
Website: www.abs.gov.au/ausstats/abs@.nsf/mf/1200.0.55.008
National best practice guidelines for collecting Indigenous status in health data sets
The website below contains links to several valuable resources including best practice guidelines created by the AIHW, which document the recommended national approach to collecting and recording Indigenous status in health services. It also contains a link to a training tool for staff in the form of a 12 question spreadsheet, designed to assess staff knowledge relating to the collection of Indigenous data.
Website: www.aihw.gov.au/reports-statistics/population-groups/indigenous-australians/links-other-information
National Indigenous Data Improvement Support Centre (NIDISC)
The NIDISC is the AIHW’s helpdesk which provides advice and help in regards to the implementation of their best practice guidelines.
Phone: 1800 223 919
Email: nidisc@aihw.gov.au
325 RCFV 2016, Volume 5 Report and recommendations, p.7.
326 Department of Health and Human Services, Dhelk Dja: Safe Our Way: Strong Culture, Strong Peoples, Strong Families,
dhhs.vic.gov.au/publications/strong-culture-strong-peoples-strong-families-10-year-plan
327 State Government of Victoria, Improve the collection of Indigenous specific data relating to family violence, viewed 22 June 2018,
www.vic.gov.au/family-violence-recommendations/improve-collection-indigenous-specific-data-relating-family
328 ABS 2014, 1200.0.55.008 Indigenous Status Standard, 2014, version 1.5, viewed 22 June 2018,
www.abs.gov.au/ausstats/abs@.nsf/mf/1200.0.55.008
329 Aboriginal Family Violence Prevention and Legal Service Victoria 2015, Submission to the Victorian Royal Commission into Family Violence, no. 941, p.22, viewed 22 June 2018, www.rcfv.com.au/Submission-Review
330 Ibid.
331 ABS 2016, 4714.0 National Aboriginal and Torres Strait Islander Social Survey, 2014-15, viewed 22 June 2018,
www.abs.gov.au/AUSSTATS/abs@.nsf/mf/4714.0
332 Aboriginal Family Violence Prevention and Legal Service Victoria 2015, Submission to the Victorian Royal Commission into Family Violence, no. 941, p.13, viewed 22 June 2018, www.rcfv.com.au/Submission-Review
333 Dwyer, J & Miller, R 2014, Working with families where an adult is violent: Best interests case practice model, Victorian Government Department of Human Services, Melbourne.
334 RCFV 2016, Volume 5 Report and recommendations, p.12.
335 Ibid p.24.
336 Aboriginal Family Violence Prevention and Legal Service Victoria 2015, Submission to the Victorian Royal Commission into Family Violence, no. 941, p.16, viewed 22 June 2018, www.rcfv.com.au/Submission-Review
337 AIHW 2018, Family, domestic and sexual violence in Australia 2018, Cat. no. FDV 2, Canberra, p.83.
338 Aboriginal Affairs Victoria 2003, Victorian Indigenous Family Violence Task Force Final Report, Department for Victorian Communities, State of Victoria, p.6.
339 RCFV 2016, Volume 5 Report and recommendations, p.10.
340 Aboriginal Family Violence Prevention and Legal Service Victoria 2015, Submission to the Victorian Royal Commission into Family Violence, no. 941, p.23, viewed 22 June 2018, www.rcfv.com.au/Submission-Review
341 AIHW 2018, Family, domestic and sexual violence in Australia 2018, Cat. no. FDV 2, Canberra, p.86.
342 Ibid.
343 Ibid p.87.
344 Aboriginal Family Violence Prevention and Legal Service Victoria 2015, Submission to the Victorian Royal Commission into Family Violence, no. 941, p.23, viewed 22 June 2018, www.rcfv.com.au/Submission-Review
345 RCFV 2016, Volume 5 Report and recommendations, p.28.
346 Ibid p.29.
347 Victorian Aboriginal Legal Service, Royal Commission into Family Violence: Submission paper from the Victorian Aboriginal Legal Service, no. 826, p.12, viewed 22 June 2018, www.rcfv.com.au/Submission-Review
348 Aboriginal Family Violence Prevention and Legal Service Victoria 2015, Submission to the Victorian Royal Commission into Family Violence, no. 941, p.53, viewed 22 June 2018, www.rcfv.com.au/Submission-Review
349 RCFV 2016, Volume 5 Report and recommendations, p.29.
350 AIHW 2010, National best practice guidelines for collecting Indigenous status in health data sets, Cat. no. IHW 29, Canberra.
351 RCFV 2016, Volume 5 Report and recommendations, p.56.
352 Ibid p.27.
353 Kelaher, M, Parry, A, Day, S, Paradies, Y, Lawlor, J & Solomon, L, 2010, Improving the Identification of Aboriginal and Torres Strait Islander People in Mainstream General Practice, The Lowitja Institute, Melbourne, p.75.
354 ABS 2014, 4733.0 Information Paper: Review of the Indigenous Status Standard, 2014, viewed 22 June 2018,
www.abs.gov.au/ausstats/abs@.nsf/Latestproducts/4733.0Main%20Features99992014?opendocument
355 Family Safety Victoria 2017, Family Violence Information Sharing Guidelines: Guidelines for Information Sharing Entities, Victorian Government, Melbourne, p.84.
356 RCFV 2016, Volume 5 Report and recommendations, p.29.
357 Ibid.
358 The FVPA defines Aboriginal and Torres Strait Islander tradition as (a) ‘the body of traditions, observances, customs and beliefs of Aboriginal and Torres Strait Islander people generally or of a particular community or group of Aboriginal and Torres Strait Islander people; and (b) any such traditions, observances, customs or beliefs relating to particular persons, areas, objects or relationships’.
359 Al-Yaman, F, Van Doeland, M, Wallis, M 2006, Family violence among Aboriginal and Torres Strait Islander peoples, Cat no. IHW 17, AIHW, Canberra.
360 ABS 2014, 1200.0.55.008 Indigenous Status Standard, 2014, version 1.5, viewed 22 June 2018,
www.abs.gov.au/ausstats/abs@.nsf/mf/1200.0.55.008
361 Ibid.
362 Ibid.
363 AIHW 2010, National best practice guidelines for collecting Indigenous status in health data sets, Cat. no. IHW 29, Canberra.
364 RCFV 2016, Volume 5 Report and recommendations, p.35.
365 Ibid p.34.
Intersectionality and family violence
Many factors combine to form an individual’s identity and experience. While this framework has looked at priority communities in discrete sections, it should be noted that identity is complex and individuals should not be categorised based on one aspect of their identity.
Many factors combine to form an individual’s identity and experience. While this framework has looked at priority communities in discrete sections, it should be noted that identity is complex and individuals should not be categorised based on one aspect of their identity. The Victorian Government’s Family Violence Diversity and Intersectionality Framework defines intersectionality as “different aspects of a person’s identity that can expose [that person] to overlapping forms of discrimination and marginalisation”.366 These aspects can include gender, class, ethnicity and cultural background, religion, disability and sexual orientation.367, 368
It is critical that family violence service providers and agencies adopt an intersectional approach. In the context of family violence, this means that services need to identify how the factors noted above can be associated with different sources of oppression and discrimination, and how those intersections can lead to increased risk, severity and frequency of experiencing different forms of violence.369 Services should appreciate the role that multiple sources of identity play in a person’s lived experiences, and be accessible, inclusive, non-discriminatory and responsive to the needs of diverse groups.
Due to the lack of existing administrative data concerning the priority communities discussed in this framework, minimal information is known about how diversity characteristics interact to compound the risk of family violence. However, some examples of how different aspects of a person’s identity can intersect to increase the risk of exposure to family violence have been outlined below. It is important to note that family violence is not part of any culture or unique to any specific community; however, the presence of power imbalances, discrimination and stigma experienced by diverse communities may heighten the risk of family violence.
Example 1. Gender inequality means that women are most at risk of experiencing family violence. The risk for women in diverse communities is exacerbated by intersecting social and institutional disadvantages, which create additional barriers to service access and disclosure. Aboriginal women are significantly more likely to be exposed to family violence and require hospitalisation for injuries than non-Aboriginal women, which may be explained by the intersection of race and gender-based discrimination and inequality.370
Example 2. Older people from CALD backgrounds who have recently migrated to Australia may experience social isolation, as they often lose their support networks through the process of relocation. They may also experience difficulties in accessing services, including facing language barriers, or having apprehension about contacting a mainstream service. As a result, older people from CALD backgrounds may become dependent on family members more fluent in English to meet their daily needs, which is problematic if these family members are responsible for perpetrating violence against them. Cultural norms and a fear of being ostracised from their family and community may prevent older CALD people from seeking help.371
Example 3. Children with disabilities are at increased risk of experiencing abuse, neglect and other forms of maltreatment, perpetrated by a parent or carer. Statistics on the victimisation of children with disabilities are limited, however, international studies have found that children with physical, sensory, intellectual and mental disabilities are twice as likely to experience violence than children that do not have disabilities.372
Example 4. Some CALD communities may hold more conservative views on gender and sexuality due to their cultural and religious backgrounds. These attitudes and beliefs may support or reinforce discrimination and violence against lesbian, gay, bisexual, transgender and intersex people. The rejection of people on the basis of their sexuality or gender, and threats of ‘outing’ someone, may be used as a form of control and abuse within some CALD communities.373
Example 5. Disabilities disproportionately affect people over the age of 65. The care needs of older people with disabilities may place time and financial pressures on family members, and create tension or conflict within the home environment. Older people with disabilities are more vulnerable to abuse as a result of the accumulated risk associated with age-related disabilities or lifelong disabilities.374
In order to understand how family violence affects people in diverse communities, data needs to be reliably and consistently collected from the priority communities included in this framework. The collection of high quality, disaggregated data from these communities will not only enhance our understanding of the experiences of people from diverse groups, but will also provide information about the impact of family violence on people from intersectional backgrounds, and the unique risks and challenges that they face.
The framework can assist Priority 1: Building Knowledge from the Everybody Matters: Inclusion and Equity Statement (Everybody Matters)375 released in April 2019. Priority 1 focuses on research and data collection to fill gaps in current knowledge. Everybody Matters highlights the need to collect data around the unique experiences of people who access the service system from early intervention to response. The framework directly aids the fulfillment of this goal.
Modified from the Equality Institute 2017, and Our Watch 2017. 367, 377
366 State Government of Victoria, Diversity and Intersectionality Framework, viewed 22 June 2018, https://www.vic.gov.au/familyviolence/designing-for-diversity-and-intersectionality/diversity-and-intersectionality-framework.html
367. Ibid.
368. Frawley, P, Dyson, S, Robinson, S & Dixon, J 2015, What does it take? Developing informed and effective tertiary responses to violence and abuse of women and girls with disabilities in Australia, Landscapes: State of knowledge no. 3, ANROWS, Alexandria.
369. The Equality Institute 2017, Preventing and responding to family violence: Taking an intersectional approach to address violence in Australian communities, viewed 22 June 2018, www.equalityinstitute.org/family-violence-primary-prevention-in-victoria/
370. State of Victoria (Department of Premier and Cabinet) & the Equality Institute 2017, Family violence primary prevention: Building a knowledge base and identifying gaps for all manifestations of family violence, viewed 22 June 2018, https://www.vic.gov.au/system/user_files/Documents/fv/Family_Violence_Primary_Prevention%20-%20Building_a_knowledge_base_and_identifying_gaps_for_alll_manifestations_of_family_violence.pdf
371. Blundell, B B & Clare, M 2012, Elder Abuse in Culturally and Linguistically Diverse Communities: Developing Best Practice, Centre for Vulnerable Children and Families: The University of Western Australia and Advocare Incorporated, Perth.
372. State of Victoria (Department of Premier and Cabinet) & the Equality Institute 2017, Family violence primary prevention: Building a knowledge base and identifying gaps for all manifestations of family violence, viewed 22 June 2018, https://www.vic.gov.au/system/user_files/Documents/fv/Family_Violence_Primary_Prevention%20-%20Building_a_knowledge_base_and_identifying_gaps_for_alll_manifestations_of_family_violence.pdf
373. Ibid.
374. Ibid.
375 Everybody Matters: Inclusion and Equity Statement, Viewed 17 April 2018, https://w.www.vic.gov.au/system/user_files/Documents/fv/Everybody%20Matters%20Inclusion%20and%20Equity%20Statement.pdf
376 The Equality Institute 2017, Preventing and responding to family violence: Taking an intersectional approach to address violence in Australian communities, viewed 22 June 2018, www.equalityinstitute.org/family-violence-primary-prevention-in-victoria/
377 Our Watch 2017, Intersectionality graphics, viewed 22 June 2018, https://www.ourwatch.org.au/getmedia/4135841b-76e8-4f11-88c4-76be0c8e12ae/Intersectionality-images.zip.aspx?ext=.zip
List of stakeholders
Provides a list of contacts who were sent a copy of the draft framework and asked to providefeedback.
The following is a list of contacts who were sent a copy of the draft framework and asked to provide feedback. It should be noted that this is not an exhaustive list, as the draft was further disseminated through channels held by certain stakeholders, including members of Domestic Violence Victoria, the Victorian Government Family Violence Steering Committee and the Diverse Communities and Intersectionality Working Group.
| Organisation | Area |
|---|---|
| Arabic Welfare | |
| Australian GLBTIQ Multicultural Council | |
| Australian Institute of Health and Welfare | Disability and Ageing |
| Australian Muslim Women's Centre for Human Rights | |
| Australian Vietnamese Women's Association | |
| Berry Street | |
| Bisexual Alliance Victoria | |
| Carers Australia Victoria | |
| Centre for Excellence in Child and Family Welfare Inc | |
| Centre for Multicultural Youth | |
| Commission for Children and Young People | |
| Coroners Court of Victoria | Crime Prevention Unit |
| Department of Education and Training | Social Cohesion and Family Violence – Wellbeing, Health and Engagement Division |
| Department of Health and Human Service |
Business Technology and Information Management Outcomes, Performance and Risk Branch – Strategy and Planning Division Health and Human Services Workforce Branch – Strategy and Planning Division Operational Performance and Quality Branch – Children, Families, Disability and Operations Division Community Based Health Policy and Programs Branch – Health and Wellbeing Division Diversity and Community Participation Branch – Health and Wellbeing Division Health Services Data – Health Data Standards and Systems Office of Professional Practice Office for Disability Mental Health Branch – Health and Wellbeing Division Disability and NDIS Branch – Children, Families, Disability and Operations Division Victorian Agency for Health Information |
| Department of Justice and Regulation |
Koori Caucus Working Group on Family Violence (members include representatives from Koori Justice Unit, Victorian Aboriginal Community Services Association, Djirra, and a number of Regional Aboriginal Justice Advisory Committees) Corrections Victoria (Modelling, Analysis and Statistics) CSA Family Violence Database Advisory Working Group |
| Department of Premier and Cabinet |
Victorian Centre for Data Insights Multicultural Affairs and Social Cohesion Division Equality Branch Commissioner for Gender and Sexuality Office for Women |
| Disability Discrimination Legal Services | |
| Disability Justice Advocacy | |
| Disability Services Commissioner | |
| Djirra (formerly the Aboriginal Family Violence Prevention and Legal Service Victoria) | |
| Domestic Violence Victoria | |
| Drummond Street Services | |
| Ethnic Community Council of Victoria | |
| Family Access Network | |
| Family Relationship Centre | |
| Family Safety Victoria |
Diversity, Engagement and Strategy Risk Management and Information Sharing System Policy and Reform Information Systems Reform |
| Federation of Community Legal Centres Victoria Inc | |
| Foundation House (Victorian Foundation for Survivors of Torture Inc) | |
| GASP Geelong | |
| Gay and Lesbian Health Victoria | |
| Health Complaints Commissioner | |
| Home of Multicultural Exchange Group | |
| inTouch Multicultural Centre against Family Violence | |
| Jewish Care | |
| Launch Housing | |
| Mental Health Complaints Commissioner | |
| Mind Australia | |
| Mind Equality Centre | |
| Monash Health | |
| Monash University | |
| Multicultural Centre for Women's Health | |
| No to Violence | Projects and Policy |
| Office of the Public Advocate | |
| Office of the Victorian Information Commissioner | |
| safe steps Family Violence Response Centre |
Policy LGBTIQA+ Family Violence Network |
| Seniors Rights Victoria | |
| South Sudanese Community in Australia | |
| Southern Melbourne Integrated Family Violence Partnership / WAYSS | |
| Spectrum VIC | |
| The Royal Children's Hospital Melbourne | |
| Transgender Victoria | |
| Victoria Legal Aid | |
| Victoria Police |
Priority Communities Division
|
| Victorian Aboriginal Child Care Agency | |
| Victorian Aboriginal Community Controlled Health Organisation | |
| Victorian Aboriginal Legal Service | |
| Victorian Aids Council | |
| Victorian Cooperative on Children's Services for Ethnic Groups | |
| Victorian Council of Social Service | |
| Victorian Gay and Lesbian Rights Lobby | |
| Victorian Multicultural Commission | |
| VicServ | |
| Women with Disabilities Victoria | |
| Women's Health In the North | |
| WoVG Information Management Group |
Department of Treasury and Finance Environmental Protection Authority |
| Wyndham Community & Education Centre | |
| Youth Disability Advocacy Service | |
| Youth Research Centre, University of Melbourne |