- Date:
- 16 July 2021
Introduction
The Foundation Knowledge Guide explains key elements of the MARAM Framework, as well as additional foundational knowledge to guide all professionals who will go on to use the MARAM Practice Guides.
This updated version of the Foundation Knowledge Guide (2021) includes information from both the victim survivor and perpetrator-focused practice lenses to provide a complete resource for all professionals and organisations with responsibilities under the MARAM Framework.
It includes evidence-based information about the effects and experiences of risk across a range of age groups, as well as in Aboriginal communities, diverse communities and at-risk age groups, including children, young people and older people.
2.1 A shared responsibility
It builds on the findings and recommendations of the Royal Commission, and most importantly, it provides the basis for a consistent, system-wide shared responsibility to identify, screen, assess and manage family violence across a broad range of workforces and services.
This shared responsibility stretches between individual professionals, services and whole sectors.
It gives services more options to keep victim survivors safe, and provides a stronger, more collaborative approach to holding perpetrators accountable for their actions and behaviours.
2.2 About this guide
The Foundation Knowledge Guide covers:
- a principles-based approach to practice
- the legislative authorising environment for practice under the MARAM Framework
- an overview of the service system, including entry points for service users (both victim survivors and perpetrators)
- guidance for organisational leaders, individual professionals and services to identify the responsibilities that make up their role, and how to use the victim-survivor and perpetrator-focused MARAM Practice Guides in their work
- information about family violence — including the definition under the Act, behaviours that constitute family violence, evidence-based risk factors and presentations of risk for victim survivors caused by perpetrators’ use of violence, across age groups, and across communities
- working with child and adult victim survivors and adult perpetrators of family violence, including concepts of the predominant aggressor and misidentification
- key concepts for practice, including structured professional judgement, intersectional analysis, trauma and violence–informed practice, person or victim-centred practice, and the legislation supporting information sharing.
Overview of the MARAM Framework and resources
Family violence is an endemic issue that has terrible consequences for individuals, families and communities in Victoria.
To address this crime and improve the complex, interconnected system of services that respond to it, the Victorian Government launched Australia’s first Royal Commission into Family Violence (the Royal Commission) in February 2015. The Royal Commission delivered its report and recommendations in March 2016.
The 227 recommendations outline a vision for a Victoria that:
- is free from family violence
- keeps adults, young people and children safe
- responds to victim survivors’ wellbeing and needs
- holds perpetrators to account for their actions and behaviours.
1.1 Reforms to risk assessment and management
In particular, the Royal Commission’s recommendations focus on providing consistent, collaborative approaches to identifying, assessing and managing family violence risk.
The Royal Commission noted the strong foundations of existing practice, which was based on the Family Violence Risk Assessment and Risk Management Framework (also known as the Common Risk Assessment Framework or CRAF).
To address key gaps and issues, however, the Royal Commission recommended redeveloping the CRAF, and embedding it into the Family Violence Protection Act 2008 (Vic) (the FVPA).
1.2 The MARAM Framework
The Victorian Family Violence Multi-Agency Risk Assessment and Management Framework (MARAM Framework) updates and replaces the CRAF.
The MARAM Framework provides a system-wide approach to risk assessment and risk management.
It aims to:
- increase the safety of people experiencing family violence
- ensure the broad range of family violence experiences and risks are represented, including for Aboriginal and diverse communities, children, young people and older people, and across identities and family and relationship types
- keep perpetrators in view of the system and hold them accountable
- align practice across the broad range of organisations that are responsible for identifying, assessing and managing family violence risk
- ensure consistent use of the framework across these organisations and between the sectors that comprise the family violence system.
To meet these aims, the MARAM Framework provides:
- 10 Framework Principles to underpin practice across the service system
- four conceptual ‘pillars’ against which organisations will align their policies, procedures, practice guidelines and tools
- 10 Responsibilities for Practice that describe the roles and expectations of framework organisations
- information to support a shared understanding of family violence, including the experience of risk and its effect on individuals, families and communities.
In addition, the MARAM Framework provides for an expanded range of organisations and sectors that have a formal role in family violence risk assessment and risk management practice.
1.3 Prescribed organisations
Under amendments to the FVPA, organisations across the many parts of the social service system must now ensure their policies, procedures, practice guidance and tools align with the MARAM Framework.
These are known as prescribed organisations.
From April 2021, organisations and professionals covered under the reforms, include:
- 6,710 organisations and 392,000 professionals will be prescribed under MARAM
- 8,386 organisations and 408,000 professionals will be prescribed under FVISS.
Ensuring prescribed organisations align their risk assessment and management activities with the MARAM Framework means there will be a consistent response to family violence across Victoria’s service system.
1.4 Risk assessment and management responsibilities
The MARAM Framework outlines the 10 practice responsibilities that prescribed organisations must adhere to in their work with victim survivors and perpetrators of family violence:
- Responsibility 1: Respectful, sensitive and safe engagement
- Responsibility 2: Identification of family violence
- Responsibility 3: Intermediate risk assessment
- Responsibility 4: Intermediate risk management
- Responsibility 5: Seek consultation for comprehensive risk assessment, risk management and referrals
- Responsibility 6: Contribute to information sharing with other services (as authorised by legislation)
- Responsibility 7: Comprehensive assessment
- Responsibility 8: Comprehensive risk management and safety planning
- Responsibility 9: Contribute to coordinated risk management
- Responsibility 10: Collaborate for ongoing risk assessment and risk management
The MARAM Practice Guides provide practical advice for people working in prescribed organisations to embed these responsibilities in their engagement with victim survivors and perpetrators.
1.5 About this document and the MARAM Practice Guides
This document, the Foundation Knowledge Guide, is part of a suite of resources known as the MARAM Practice Guides.
These resources comprise:
- this Foundation Knowledge Guide
- MARAM Practice Guides that show you how to implement the Responsibilities in your work
- risk assessment and management tools and templates that support the MARAM Practice Guides
- the Organisation Embedding Guidance and Resources to support organisational leaders.
A MARAM Practice Guide for adolescents who use violence is currently under development.
The MARAM Framework and Practice Guides were developed through extensive consultation with experts, departmental policy and practice areas, and professionals in specialist and universal services, including those specialising in working with Aboriginal communities, diverse communities, children, young people and older people.
The MARAM Framework and Practice Guides will be evaluated and updated as the evidence base evolves.
1.5.1 Foundation Knowledge Guide
The Foundation Knowledge Guide isfor all practitioners who use the MARAM Framework.
It focuses on the legislative context, roles and interactions within the service system, risk factors, key concepts for practice, and an overview of the gendered lens and drivers of family violence and presentations of risk across different age groups and Aboriginal and diverse communities.
The Foundation Knowledge Guide is required reading for all professionals across leadership and governance, management and supervision to direct practice roles.
You should read it first before moving on to the relevant victim–survivor or perpetrator-focused MARAM Practice Guides 1–10.
1.5.2 MARAM Practice Guides
The MARAM Practice Guides each comprise 10 chapters relating to the 10 MARAM Responsibilities. They are for professionals working with adult and child victim survivors of family violence, and adult perpetrators of family violence:
- Responsibilities for Practice Guide when working with adult and child victim survivors of family violence (2019), referred to as the victim survivor–focused MARAM Practice Guide
- Responsibilities for Practice Guide when working with adults using family violence (2021), referred to as the perpetrator-focused MARAM Practice Guide.
There is some overlap in content between the two sets of guides, as many of the same principles and practice concepts apply to working with both victim survivors and perpetrators.
Each guide gives you detailed advice on how to ensure your practice aligns with your organisation’s MARAM Framework responsibilities.
The guides cover applying foundation knowledge, and then build on this to provide practice guidance for:
- safe engagement
- identification of risk
- levels of risk assessment and management
- secondary consultation and referral
- information sharing
- multiagency and coordinated practice.
Different professionals within prescribed organisations will have different levels of responsibility, which will be informed by the contact they have with victim survivors and perpetrators.
You should work with your organisational leaders to understand your role and to identify which responsibilities to apply in practice.
You must understand how to apply each of the responsibilities that are a part of your role.
Note: Guidance on working with adolescents and young people as victim survivors is provided in the victim survivor–focused MARAM Practice Guide. Supplementary guidance for working with adolescents who use family violence will be published in 2024.
Young people aged 18 to 25 years should be considered with a developmental lens and to ensure any therapeutic needs relevant to their age and developmental stage are met. The adult perpetrator-focused MARAM Practice Guide has relevant information for assessing and managing risk when working with young people aged 18 to 25 years who use family violence.
Supplementary guidance for working with children and young people to directly and comprehensively assess risk and needs will be published in 2024.
1.5.3 Organisation Embedding Guidance and Resources
The Organisation Embedding Guidance and Resources are for organisational leaders. It aims to help leaders support their professionals and services in their roles and responsibilities under the MARAM Framework.
It includes specific activities organisational leaders can undertake to determine responsibilities for staff across their organisation.
Evidence-based risk factors and the MARAM risk assessment tools
There are 3 categories of risk factors under the MARAM Framework.
Comprising those that are:
- specific to an adult victim survivor’s circumstances
- caused by a perpetrator’s behaviour towards an adult or child victim survivor
- additional risk factors caused by a perpetrator’s behaviour specific to children, which recognises that children experience some unique risk factors, and that their risk must be assessed independently of adult victim survivors.
There is also a separate category reflecting children’s circumstances that may indicate (not determine in isolation) that family violence is present or escalating and should prompt assessment of children.
The risk factors reflect the current and emerging evidence base relating to family violence risk.
International evidence-based reviews[27] and consultation with academics and expert professionals have informed the development of a range of evidence-based risk factors that signal that family violence may be occurring.
This practice guidance is concerned with risk factors associated with an adult perpetrator’s family violence behaviours towards adult and child victim survivors.
Each perpetrator’s patterns of behaviour towards adult and child victim survivor(s) can be understood as coercive and controlling behaviour, or coercive control.
Perpetrators exert coercive control using a range of behaviours over time, and their effect is cumulative.
Coercive control can be exerted through any combination or pattern of the evidence-based risk factors.
It is often demonstrated through patterned behaviours of emotional, financial abuse and isolation, stalking (including monitoring of technology), controlling behaviours, to choking/strangulation, sexual and physical violence.
One occurrence of family violence behaviour can create the dynamic of ongoing coercion or control, due to the threat of possible future family violence behaviour and the resultant ongoing fear, even if ‘high-risk’ behaviours do not re-occur.
The implication for professionals working with perpetrators of family violence is that narratives and behaviours that appear innocuous may in fact be part of a pattern of behaviour making victim survivors feel unsafe and elevating their level of risk.
In addition, understanding adult and child victim survivors’ and perpetrators’ broader needs and circumstances can help you to identify, assess and manage risk according to your level of MARAM responsibility.
In Table 3, emerging evidence-informed family violence risk factors are indicated with a hash (#).
Serious risk factors — those that may indicate an increased risk of the victim being killed or almost killed — are highlighted with orange shading##.
Table 3: Evidence-based risk factors
|
Risk factors relevant to an adult victim’s circumstances |
Explanation |
|---|---|
|
Physical assault while pregnant/following new birth |
Family violence often commences or intensifies during pregnancy and is associated with increased rates of miscarriage, low birth weight, premature birth, foetal injury and foetal death. Family violence during pregnancy is regarded as a significant indicator of future harm to the woman and child victim. This factor is associated with control and escalation of violence already occurring. |
|
Self-assessed level of risk |
Victims are often good predictors of their own level of safety and risk, including as a predictor of re-assault. Professionals should be aware that some victims may communicate a feeling of safety, or minimise their level of risk, due to the perpetrator’s emotional abuse tactics creating uncertainty, denial or fear, and may still be at risk. |
|
Planning to leave or recent separation |
For victims who are experiencing family violence, the high-risk periods include when a victim starts planning to leave, immediately prior to taking action, and during the initial stages of or immediately after separation. Victims who stay with the perpetrator because they are afraid to leave often accurately anticipate that leaving would increase the risk of lethal assault. Victims (adult or child) are particularly at risk during the first two months of separation. |
|
Escalation - increase in severity and/or frequency of violence |
Violence occurring more often or becoming worse is associated with increased risk of lethal outcomes for victims. |
|
Imminence |
Certain situations can increase the risk of family violence escalating in a very short timeframe. The risk may relate to court matters, particularly family court proceedings, release from prison, relocation, or other matters outside the control of the victim which may imminently impact their level of risk. |
|
Financial abuse/difficulties |
Financial abuse (across socioeconomic groups), financial stress and gambling addiction, particularly of the perpetrator, are risk factors for family violence. Financial abuse is a relevant determinant of a victim survivor staying or leaving a relationship. |
|
Risk factors for adult or child victim survivors caused by perpetrator behaviours |
Explanation |
|
Controlling behaviours |
Use of controlling behaviours is strongly linked to homicide. Perpetrators who feel entitled to get their way, irrespective of the views and needs of, or impact on, others are more likely to use various forms of violence against their victim, including sexual violence. Perpetrators may express ownership over family members as an articulation of control. Examples of controlling behaviours include the perpetrator telling the victim how to dress, who they can socialise with, what services they can access, limiting cultural and community connection or access to culturally appropriate services, preventing work or study, controlling their access to money or other financial abuse, and determining when they can see friends and family or use the car. Perpetrators may also use third parties to monitor and control a victim or use systems and services as a form of control over a victim, such as intervention orders and family court proceedings. |
|
Access to weapons |
A weapon is defined as any tool or object used by a perpetrator to threaten or intimidate, harm or kill a victim or victims, or to destroy property. Perpetrators with access to weapons, particularly guns and knives, are much more likely to seriously injure or kill a victim or victims than perpetrators without access to weapons. |
|
Use of weapon in most recent event |
Use of a weapon indicates a high level of risk because previous behaviour is a likely predictor of future behaviour. |
|
Has ever harmed or threatened to harm victim or family members |
Psychological and emotional abuse are good predictors of continued abuse, including physical abuse. Previous physical assaults also predict future assaults. Threats by the perpetrator to hurt or cause actual harm to family members, including extended family members, in Australia or overseas, can be a way of controlling the victim through fear. |
|
Has ever tried to strangle or choke the victim |
Strangulation or choking is a common method used by perpetrators to kill victims. It is also linked to a general increased lethality risk to a current or former partner. Loss of consciousness, including from forced restriction of airflow or blood flow to the brain, is linked to increased risk of lethality (both at the time of assault and in the following period of time) and hospitalisations, and of acquired brain injury. |
|
Has ever threatened to kill victim |
Evidence shows that a perpetrator’s threat to kill a victim (adult or child) is often genuine and should be taken seriously, particularly where the perpetrator has been specific or detailed, or used other forms of violence in conjunction to the threat indicating an increased risk of carrying out the threat, such as strangulation and physical violence. This includes where there are multiple victims, such as where there has been a history of family violence between intimate partners, and threats to kill or harm another family member or child/children. |
|
Has ever harmed or threatened to harm or kill pets or other animals |
There is a correlation between cruelty to animals and family violence, including a direct link between family violence and pets being abused or killed. Abuse or threats of abuse against pets may be used by perpetrators to control family members. |
|
Has ever threatened or tried to self-harm or commit suicide |
Threats or attempts to self-harm or commit suicide are a risk factor for murder–suicide. This factor is an extreme extension of controlling behaviours. |
|
Stalking of victim |
Stalkers are more likely to be violent if they have had an intimate relationship with the victim, including during, following separation and including when the victim has commenced a new relationship. Stalking when coupled with physical assault, is strongly connected to murder or attempted murder. Stalking behaviour and obsessive thinking are highly related behaviours. Technology-facilitated abuse, including on social media, surveillance technologies and apps is a type of stalking. |
|
Sexual assault of victim |
Perpetrators who sexually assault their victim (adult or child) are also more likely to use other forms of violence against them. |
|
Previous or current breach of court orders/intervention orders |
Breaching an intervention order, or any other order with family violence protection conditions, indicates the accused is not willing to abide by the orders of a court. It also indicates a disregard for the law and authority. Such behaviour is a serious indicator of increased risk of future violence. |
|
History of family violence |
Perpetrators with a history of family violence are more likely to continue to use violence against family members and in new relationships. |
|
History of violent behaviour (not family violence) |
Perpetrators with a history of violence are more likely to use violence against family members. This can occur even if the violence has not previously been directed towards family members. The nature of the violence may include credible threats or use of weapons and attempted or actual assaults. Perpetrators who are violent men generally engage in more frequent and more severe family violence than perpetrators who do not have a violent past. A history of criminal justice system involvement (for example, amount of time and number of occasions in and out of prison) is linked with family violence risk. |
|
Obsession/jealous behaviour toward victim |
A perpetrator’s obsessive and/or excessive behaviour when experiencing jealousy is often related to controlling behaviours founded in rigid beliefs about gender roles and ownership of victims and has been linked to violent attacks. |
|
Unemployed / Disengaged from education |
A perpetrator’s unemployment is associated with an increased risk of lethal assault, and a sudden change in employment status — such as being terminated and/or retrenched — may be associated with increased risk. Disengagement from education has similar associated risks to unemployment. |
|
Drug and/or alcohol misuse/abuse |
Perpetrators with a serious problem with illicit drugs, alcohol, prescription drugs or inhalants can lead to impairment in social functioning and creates an increased risk of family violence. This includes temporary drug-induced psychosis. |
|
Mental illness / Depression |
Murder–suicide outcomes in family violence have been associated with perpetrators who have mental illness, particularly depression. Mental illness may be linked with escalation, frequency and severity of violence. |
|
Isolation |
A victim is more vulnerable if isolated from family, friends, their community (including cultural) and the wider community and other social networks. Isolation also increases the likelihood of violence and is not simply geographic. Other examples of isolation include systemic factors that limit social interaction or facilitate the perpetrator not allowing the victim to have social interaction. |
|
Physical harm |
Physical harm is an act of family violence and is an indicator of increased risk of continued or escalation in severity of violence. The severity and frequency of physical harm against the victim, and the nature of the physical harm tactics, informs an understanding of the severity of risk the victim may be facing. Physical harm resulting in head trauma is linked to increased risk of lethality and hospitalisations, and of acquired brain injury. |
|
Emotional abuse |
Perpetrators’ use of emotional abuse can have significant impacts on the victim’s physical and mental health. Emotional abuse is used as a method to control the victim and keep them from seeking assistance. |
|
Property damage |
Property damage is a method of controlling the victim, through fear and intimidation. It can also contribute to financial abuse, when property damage results in a need to finance repairs. |
|
Risk factors specific to children caused by perpetrator behaviours |
Explanation |
|
Exposure to family violence |
Children are impacted, both directly and indirectly, by family violence, including the effects of family violence on the physical environment or the control of other adult or child family members.[28] Risk of harm may be higher if the perpetrator is targeting certain children, particularly non-biological children in the family. Children’s exposure to violence may also be direct, include the perpetrator’s use of control and coercion over the child, or physical violence. The effects on children experiencing family violence include impacts on development, social and emotional wellbeing, and possible cumulative harm. |
|
Sexualised behaviours towards a child by the perpetrator |
There is a strong link between family violence and sexual abuse. Perpetrators who demonstrate sexualised behaviours towards a child are also more likely to use other forms of violence against them, such as:[29]
Child sexual abuse also includes circumstances where a child may be manipulated into believing they have brought the abuse on themselves, or that the abuse is an expression of love, through a process of grooming. |
|
Child intervention in violence |
Children are more likely to be harmed by the perpetrator if they engage in protective behaviours for other family members or become physically or verbally involved in the violence. Additionally, where children use aggressive language and behaviour, this may indicate they are being exposed to or experiencing family violence. |
|
Behaviour indicating non return of child |
Perpetrator behaviours including threatening or failing to return a child can be used to harm the child and the affected parent.[30] This risk factor includes failure to adhere to, or the undermining of, agreed childcare arrangements (or threatening to do so), threatened or actual removal of children overseas, returning children late, or not responding to contact from the affected parent when children are in the perpetrator’s care. This risk arises from or is linked to entitlement-based attitudes and a perpetrator’s sense of ownership over children. The behaviour is used as a way to control the adult victim, but also poses a serious risk to the child’s psychological, developmental and emotional wellbeing. |
|
Undermining the child–parent relationship |
Perpetrators often engage in behaviours that cause damage to the relationship between the adult victim and their child/children. These can include tactics to undermine capacity and confidence in parenting and undermining the child–parent relationship, including manipulation of the child’s perception of the adult victim. This can have long-term impacts on the psychological, developmental and emotional wellbeing of the children, and it indicates the perpetrator’s willingness to involve children in their abuse. |
|
Professional and statutory intervention |
Involvement of Child Protection, counsellors, or other professionals indicates that the violence has escalated to a level where intervention is required and indicates a serious risk to a child’s psychological, developmental and emotional wellbeing. |
|
There is evidence that the following child circumstance factors may indicate the presence or escalation of family violence risk. If any of these are present, you should undertake an assessment of risk for children. |
|
|
Risk factors specific to children’s circumstances |
Explanation |
|
History of professional involvement and/or statutory intervention |
A history of involvement of Child Protection, youth justice, mental health professionals, or other relevant professionals may indicate the presence of family violence risk, including that family violence has escalated to the level where the child requires intervention or other service support.[31] |
|
Change in behaviour not explained by other causes |
A change in the behaviour of a child that cannot be explained by other causes may indicate presence of family violence or an escalation of risk of harm from family violence for the child or other family members. Children may not always verbally communicate their concerns, but may change their behaviours to respond to and manage their own risk, which may include responses such as becoming hypervigilant, aggressive, withdrawn or overly compliant. |
|
Child is a victim of other forms of harm |
Children’s exposure to family violence may occur within an environment of polyvictimisation. Child victims of family violence are also particularly vulnerable to further harm from opportunistic perpetrators outside the family, such as harassment, grooming and physical or sexual assault. Conversely, children who have experienced these other forms of harm are more susceptible to recurrent victimisation over their lifetimes, including family violence, and are more likely to suffer significant cumulative effects. Therefore, if a child is a victim of other forms of harm, this may indicate an elevated family violence risk. |
9.1 Using assessment tools to identify and assess risk to victim survivors
The risk factors above are central to the identification, screening and assessment processes of Responsibilities 2, 3 and 7outlined in the MARAM Practice Guides.
Identification and screening with victim survivors helps you understand if risk is present, and to decide whether an immediate response is required.
Family violence risk assessment is used to understand the presentation of risk (what risk factors or ‘behaviours’ are being used by a perpetrator) and to determine level of risk. This is informed by analysing the presence and ‘seriousness’ of evidence-based risk factors and pattern of coercive control via a MARAM risk assessment tool.
The evidence-based risk factors are associated with family violence occurring and/or strongly linked to the likelihood of a perpetrator killing or seriously injuring a victim survivor.
In addition, the victim survivor–focused MARAM Practice Guides describe how risk factors might be experienced in Aboriginal communities, diverse communities and for older people, children and young people. The victim survivor–focused risk assessment tools provide specific questions tailored to these communities to help determine if risk factors are present.
For example, for people with disabilities, the comprehensive assessment tool asks whether anyone in the person’s family has used their disability against them (a manifestation of the ‘controlling behaviours’ risk factor for people with disabilities).
New evidence will emerge as professionals use the MARAM assessment tools and Practice Guides, which account for a broad range of experiences across the spectrum of seriousness and presentations of risk.
This will inform continuous improvement and practice change through future updates to the MARAM Framework and Practice Guides.
9.2 Using assessment tools to identify and assess risk by perpetrators
Victim survivor safety is the primary consideration when working with perpetrators.
When identifying and assessing the risk presented by perpetrators, professionals use their understanding of how family violence risk factors and patterns of family violence behaviours are targeted towards, and experienced by, adult and child victim survivors.
The MARAM risk factors also underpin the design of the perpetrator-focused identification and assessment tools under Responsibilities 2, 3 and 7 of the perpetrator-focused MARAM Practice Guides.
A person’s narratives, behaviours, presenting needs and circumstances can support identification of indicators or risk factors demonstrating their use of family violence behaviours.
The perpetrator-focused risk identification and assessment tools support observation, information gathering, contextualisation of presenting needs and circumstances and processes for direct assessment of the perpetrator, without colluding with or minimising or justifying their use of violence. The assessment tools also enable identification of patterns of coercive and controlling behaviours, points of escalation and opportunities for intervention.
In addition, these tools support information sharing to ensure the experience of the victim survivor is central to assessing the level of risk and developing risk management interventions.
You should determine victim survivors’ identity, circumstances, impacts of disadvantage or lived experience in order to understand how perpetrators may target these as part of their pattern of coercive controlling behaviour.
You should also be aware that perpetrators’ own lives are complex, and they may have had experiences of family violence (for example, when they were children) and other forms of discrimination and oppression.
Understanding perpetrators in their context is important to support more accurate identification, risk assessment and tailored risk management plans.
A principles-based approach to practice
The MARAM Framework, Foundation Knowledge Guide and victim-survivor and perpetrator-focused MARAM Practice Guides are guided by 10 MARAM Principles.
These principles provide professionals and services with a shared understanding of family violence. They will ensure consistent, effective and safe family violence responses for adult and child victim survivors as well as adult perpetrators, while centralising perpetrator accountability.
The principles are underpinned by the right of all people to live free from family violence. They inform the ethical engagement of professionals and services working with all service users, both victim survivors and perpetrators.
The 10 principles are:
- Family violence involves a spectrum of seriousness of risk and presentations, and is unacceptable in any form, across any community or culture.
- Professionals should work collaboratively to provide coordinated and effective risk assessment and management responses, including early intervention when family violence first occurs to avoid escalation into crisis and additional harm.
- Professionals should be aware, in their risk assessment and management practice, of the drivers of family violence, predominantly gender inequality, which also intersect with other forms of structural inequality and discrimination.
- The agency, dignity and intrinsic empowerment of victim survivors must be respected by partnering with them as active decision-making participants in risk assessment and management, including being supported to access and participate in justice processes that enable fair and just outcomes.
- Family violence may have serious impacts on the current and future physical, spiritual, psychological, developmental and emotional safety and wellbeing of children, who are directly or indirectly exposed to its effects, and should be recognised as victim survivors in their own right.
- Services provided to child victim survivors should acknowledge their unique experiences, vulnerabilities and needs, including the effects of trauma and cumulative harm arising from family violence.
- Services and responses provided to people from Aboriginal communities should be culturally responsive and safe, recognising Aboriginal understanding of family violence and rights to self-determination and self-management, and take account of their experiences of colonisation, systemic violence and discrimination and recognise the ongoing and present day impacts of historical events, policies and practices.
- Services and responses provided to diverse communities and older people should be accessible, culturally responsive and safe, service-user centred, inclusive and non-discriminatory.
- Perpetrators should be encouraged to acknowledge and take responsibility to end their violent, controlling and coercive behaviour, and service responses to perpetrators should be collaborative and coordinated through a system-wide approach that collectively and systematically creates opportunities for perpetrator accountability.
- Family violence used by adolescents is a distinct form of family violence and requires a different response to family violence used by adults, because of their age and the possibility that they are also victim survivors of family violence.
3.1 Principles for working with perpetrators
As a result of recommendations from the Royal Commission, the Victorian Government formed the Expert Advisory Committee on Perpetrator Interventions (EACPI) to provide advice on how to increase accountability of family violence perpetrators.
In its final report, the EACPI outlines eight principles for perpetrator interventions.
These are consistent with and supplement the MARAM Principles. They provide for a strong victim-focused lens and support perpetrator accountability at the individual, service and systems level.
The EACPI principles also inform ethical practice of professionals in their engagement with all service users.
They ensure that victim survivor safety is the key consideration when working directly with perpetrators to address their risk and needs.
Legislative, policy and practice environments
The MARAM Framework is embedded in Victorian law and policy.
It establishes the architecture and accountability mechanisms of a system-wide approach to, and shared responsibility for, responding to the family violence risk that perpetrators cause.
These elements are set at the organisational level.
They provide the authorising environment, and enablers of practice, for individual professionals and services within organisations in their work with adult and child victim survivors and adult perpetrators.
4.1 Key aspects of the MARAM Framework
- Part 11 of the Family Violence Protection Act 2008 (FVPA) establishes the authorising environment for the MARAM Framework by creating a legislative instrument and enabling prescription of organisations through regulation.
- The Framework’s legislative instrument describes the four pillars, the requirements for alignment, the guiding principles, the 10 Responsibilities for practice, and the evidence-based risk factors.
- ‘Framework organisations’ and ‘section 191 agencies’ are prescribed under the Family Violence Protection (Information Sharing and Risk Management) Regulations 2018. Prescribed organisations are required to progressively align their policies, procedures, practice guidance and tools with the Framework legislative instrument.
- The MARAM Framework complements and provides further information about the legislative instrument.
4.2 Information Sharing Schemes
The Family Violence Information Sharing Scheme is a key enabler of the MARAM Framework and associated Practice Guides.
- Part 5A of the FVPA establishes the Family Violence Information Sharing Scheme, which allows prescribed organisations to share information relevant to family violence risk assessment and management practice, in relation to victim survivor and perpetrator-focused Responsibilities 5 and 6.
- The Family Violence Information Sharing Scheme Guidelines outline how information is to be shared in practice.
The Child Information Sharing Scheme further assists in responding to safety and wellbeing for children.
- Part 6A of the Child Wellbeing and Safety Act 2005 (Vic.) establishes the Child Information Sharing Scheme, which allows the sharing of information for the purpose of promoting a child’s wellbeing or safety, including but not limited to the context of family violence. This may include information relating to a child’s stabilisation and recovery from family violence, reflected in the protective factors outlined in victim survivor–focused Responsibility 3.
Other complementary information sharing and reporting obligations continue to apply.
- The Information Sharing Schemes do not affect the reporting obligations created under other legislation, such as mandatory reporting under the Children, Youth and Families Act 2005 (Vic.).
- The Information Sharing Schemes complement and build on existing permissions held by organisations and services to share information under other laws, such as the Privacy and Data Protection Act 2014 (Vic.), the Health Records Act 2001 (Vic.), and the Children Youth and Families Act 2005 (Vic.).
4.3 Policy and practice direction
The MARAM Framework and Practice Guides, including this Foundation Knowledge Guide, provide policy and practice direction.
They are for professionals and leaders working within prescribed organisations and services that undertake family violence risk assessment and risk management practice in Victoria.
Leaders of prescribed organisations make decisions at the organisational level to identify the practice responsibilities for their professionals and services and ensure they are applied in practice.
Professionals need to have a clear understanding of their own role in relation to responding to family violence within the broader service system.
This will help to determine which level of risk identification, assessment and management applies to your role and which MARAM Responsibilities and Practice Guides are relevant to your work.
More detail on the legislative, policy and practice environment is described in ‘Part B: System architecture and accountability’ of the MARAM Framework.
4.4 The MARAM Framework Pillars
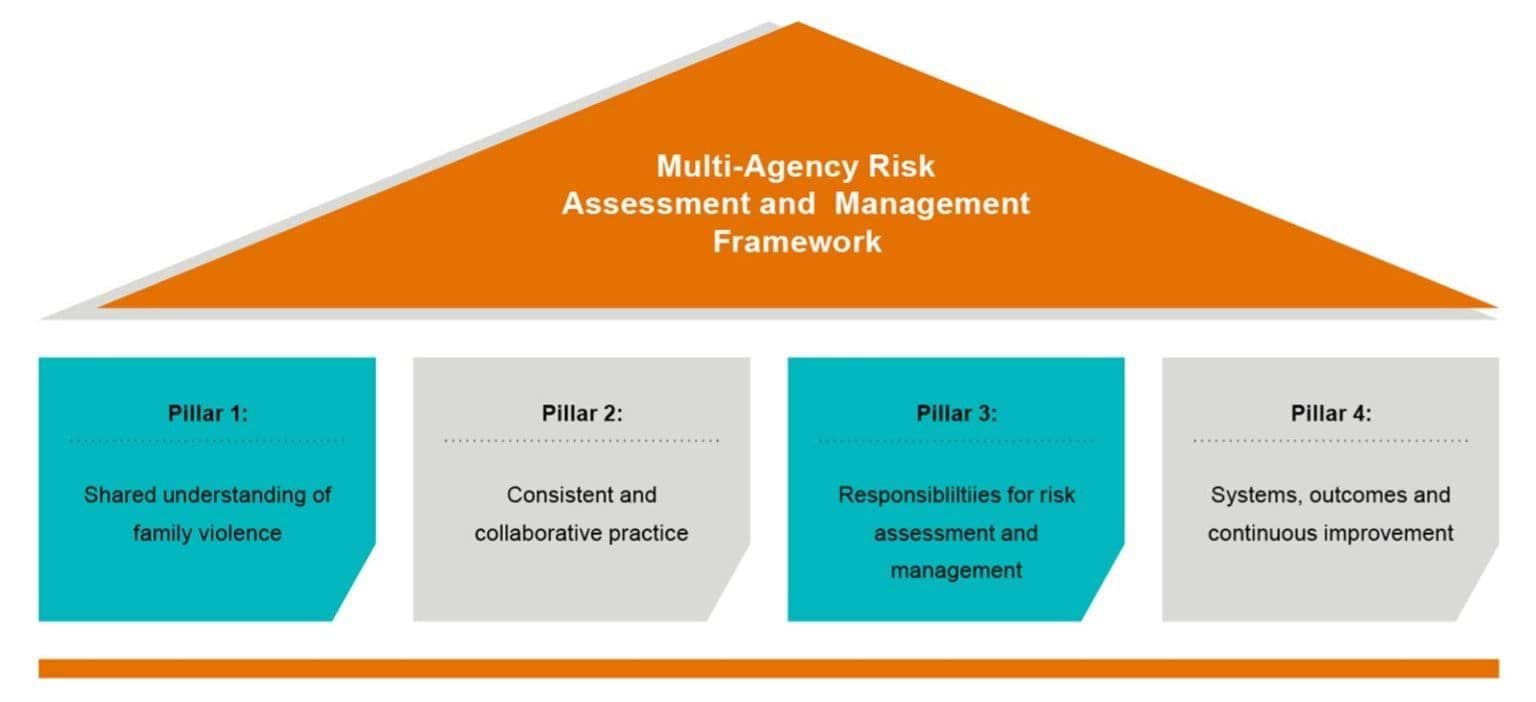
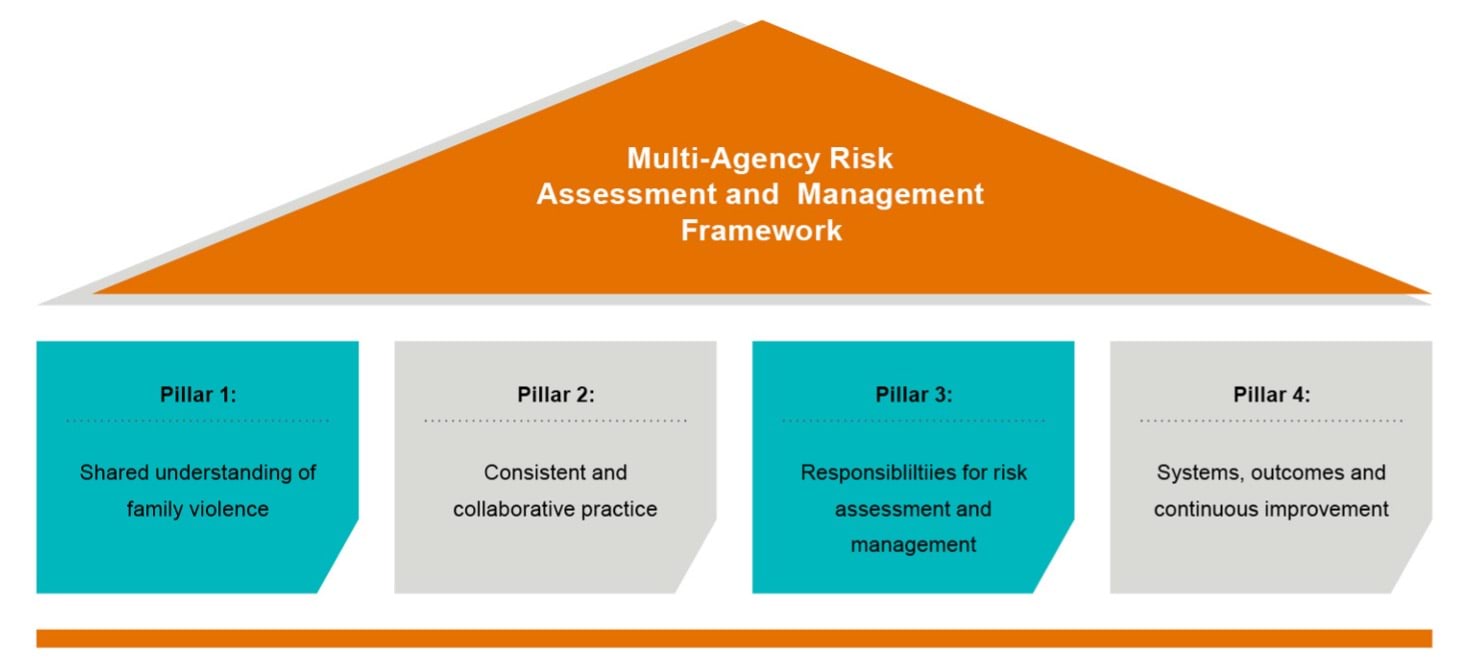
The MARAM Framework is structured around four conceptual pillars. Organisations will align their risk assessment and management policies, procedures, practice guidelines and tools with these pillars.
Each pillar has its own objective and requirement for alignment. The objectives of the pillars are outlined below.
Figure 1: MARAM Framework Pillars
{kind=link}
4.4.1 Pillar 1: Shared understanding of family violence
Everyone working in the service system, regardless of their role, needs to have a shared understanding of family violence and perpetrator behaviour, including its drivers, presentation, prevalence and impacts.
This enables a consistent approach to risk assessment and management across the service system and helps keep perpetrators in view and accountable and victim survivors safe.
Pillar 1 creates a shared understanding of:
- what constitutes family violence, including common perpetrator actions, behaviours and patterns of coercion and control
- the causes of family violence, particularly community attitudes about gender, and other forms of inequality and discrimination
- established evidence-based risk factors, particularly those that relate to increased likelihood and severity of family violence.
4.4.2 Pillar 2: Consistent and collaborative practice
Pillar 2 builds on the shared understanding of family violence created in Pillar 1 by developing consistent and collaborative practice for family violence risk assessment and management across different professional roles and sectors.
You should use Structured Professional Judgement in your role to assess the level or ‘seriousness’ of risk, informed by:
- the victim survivor’s self-assessed level of risk
- evidence-based risk factors (using the relevant assessment tool)
- sharing information with other professionals as appropriate to help inform professional judgement and decision-making
- using an intersectional analysis when applying professional judgement to determine the level of risk.
4.4.3 Pillar 3: Responsibilities for risk assessment and management
Pillar 3 builds on Pillars 1 and 2. It describes responsibilities for facilitating family violence risk assessment and management.
It provides advice on how professionals and organisations define their responsibilities to support consistency of practice across the service system, and to clarify the expectations of different organisations, professionals and service users.
4.4.4 Pillar 4: Systems, outcomes and continuous improvement
Pillar 4 outlines how organisational leaders and governance bodies contribute to, and engage with, system-wide data collection, monitoring and evaluation of tools, processes and implementation of the Framework.
This pillar describes how aggregated data will support better understanding of service user outcomes and systemic practice issues, and it will assist in continuous practice improvement.
This information will also feed into the legislated five-yearly reviews of the Framework to ensure it continues to reflect evidence-based best practice.
Terminology and definitions
Language relating to family violence and individual identities is always evolving and can vary for individuals and communities.
Language relating to family violence and individual identities is always evolving and can vary for individuals and communities.
As practitioners, it is important to use language that service users are comfortable with. This helps build trust and keep the person engaged.
This section provides guidance about some commonly used terminology. The MARAM Practice Guides also contain information on identity that will help you talk to service users.
Throughout this guide, the term Aboriginal people is used to refer to both Aboriginal and Torres Strait Islander peoples.
The terms diverse communities and at-risk age groups are used broadly, and include:
- diverse cultural, linguistic and faith communities
- people with disability
- people experiencing mental health issues
- LGBTIQ people
- women in or exiting prison or forensic institutions
- people who work in the sex industry
- people living in regional, remote and rural communities
- male victim survivors
- older people (aged 65 years and older, or 45 years and older for Aboriginal people)
- children (0 to 4 years of age are most at risk) and young people (12 to 25 years of age).
A full list of definitions is provided at the end of this document in Section 14, ‘Definitions’.
5.1 Language around gender
The MARAM Practice Guides use an intersectional analysis and feminist lens, which strongly acknowledge that family violence is gendered.
However, gendered language is not used to describe every form of family violence. This is to ensure we encompass the full range of victim survivors who may experience family violence, including those who may have historically had difficulty being recognised.
In line with the Royal Commission and the Family Violence Information Sharing Scheme Guidelines, this document and the MARAM Practice Guides refer to victim survivors and perpetrators (or person using violence),recognising that these are the most widely used terms in the community.
The term victim survivor refers to adults, children and young people who experience family violence.
Under the FVPA, children are considered victim survivors if they experience family violence directed at them, or they are exposed directly to family violence and/or its effects.
Women who use force describes victim survivors who, in their intimate partner relationships, have used force in response to violence where there is a pattern and history of ongoing perpetration of violence against them.[1] This may sometimes be referred to as ‘violent resistance’ or ‘resistive violence’. Section 12.1.13 on ‘Women who use force in heterosexual intimate partner relationships’ provides further guidance.
Some women who use force who are victim survivors do not identify as victims, because this does not match with their experience as ‘strong’ or ‘weak’, and their use of force may be in response to pushing back against a ‘weaker’ identity of victim survivor.[2]
Women who use force in response to a pattern of family violence and coercive control from a perpetrator/predominant aggressor are not themselves perpetrators. However, if you are uncertain about the identity of a victim survivor or predominant aggressor/perpetrator, refer to Section 12.2.1, ‘Perpetrator/predominant aggressor and misidentification’.
5.2 Variations of language
Recognised variations of language include the following:
- Aboriginal people and communities may prefer to use the term people who use violence rather than perpetrator.
- Aboriginal people and communities may prefer to use the term people who experience violence rather than victim survivor.
- Parts of the service system use the term men who use violence rather than perpetrator, particularly in client/service user–facing practice settings that work exclusively with men.
- For adolescents and young people, the term adolescent or young person who uses family violence is used, rather than perpetrator. This form of family violence requires a distinct response, given the age and developmental stage of the young person and their concurrent safety and developmental needs and circumstances. In addition, it is common for the adolescent or young person to have experiences of past or current family violence perpetrated by other family members. The term is applied across a broad age range from 10 to 18 years.
- Family violence towards an older person is often described as elder abuse. In this document, elder abuse refers to family violence experienced by older people within the family or family-like contexts, including co-resident violence in residential care services and supported residential settings, as it is defined in the FVPA. It does not extend to elder abuse from professional carers occurring outside the family context, such as in institutional or community settings.
- Family violence towards or between persons with a disability or a young person within the family or family-like relationships, such as residential care facilities, is included as it is defined in the FVPA. It does not extend to professional carer relationships outside of the family context, such as in institutional settings.
5.3 Language used in the justice system
Other terms may be used for different functions or points in time within the service system.
These include terms used in the justice system:
- Police-made applications for family violence intervention orders use the term affected family member to describe the person who is to be protected by the order, and the term respondent or other party to describe the person against whom the order is sought.
- In applications for intervention orders that are not made by police, the term applicant is used to describe the person seeking the order who may be an affected family member or another person making the application on their behalf, and respondent is used to describe the person against whom an order is sought.
- The term accused is used to describe a person being prosecuted for a family violence offence, and offender describes a person who has been found guilty of an offence.
5.4 Language relating to perpetrators
The term person using family violence is used through this guide and the MARAM Practice Guides to refer to the person causing family violence harm.
The term perpetrator is used at a legal and policy level in Victoria. The term is used in this guide in relation to policy statements.
When discussing violence across a range of identities and communities, the terms men who use family violence and/or person using family violence can be used, as applicable.
In direct practice with a person using violence, you should not use the term perpetrator. It is a label that de-emphasises the person’s agency for change, and in practice it may make them feel judged and more hostile or resistant to engaging with you.
If you are working with adult and child victim survivors, they may not feel comfortable with the use of the word perpetrator when they are seeking support. Understanding and mirroring the words a victim survivor uses to describe their parent, partner, ex-partner, or family member is also an important part of the engagement process in direct practice.
In addition, the use of the term perpetrator can limit your own capacity to understand or consider the person in their context, that is their presenting needs, history and experiences, risks, strengths and environmental contexts or circumstances that contribute to their use of violence. This label may also impact professionals’ capacity to apply an intersectional lens and adopt trauma and violence–informed approaches (where appropriate).
The term perpetrator accountability[3] refers to systemic legislative and policy responses that keep perpetrators in view of the service system and held to account for their behaviour. It also refers to how an individual can take personal accountability for safety and change.
This term encompasses a range of actions and approaches that occur at the:
- the individual level (by and with the person using violence) it means that perpetrators are encouraged to take responsibility for their use of violence and its impacts and to change their behaviour to stop using violence.
- the service level (by professionals in applying accountability in practice through risk assessment and management of the person using violence) it means that wherever perpetrators interact with the service system, the primary consideration is to support the safety, wellbeing and needs of victim survivors, and to avoid collusion while providing support for perpetrators to gain awareness, take responsibility and engage in positive behaviour change.
- system level (system-wide policy or direct interventions or other accountability measures) it means there is a collective responsibility to keep perpetrators ‘in view’. This ensures that perpetrators’ use of violence and control is seen as unacceptable at a community level, and there are clear consequences for family violence, underpinned by legislation and compliance measures.
Perpetrator accountability includes:
- understanding and responding to the needs of victim survivors, their experiences of perpetrators’ use of violence, and their views about the outcomes they are seeking to achieve
- prioritising women and children’s safety through effective, coordinated and ongoing risk assessment and management[4]
- encouraging perpetrators to take responsibility for their actions, including the impact of their actions on family members such as intimate partners and their children
- providing options to assist perpetrators to gain insight into and awareness of their actions and change their behaviour, tailored to their risk profile
- a strong set of laws and legal processes that impose clear consequences and sanctions for perpetrators' violent and abusive behaviour and failure to comply with police interventions and court orders
- fostering collective responsibility among government and non-government agencies, the community and individuals for denouncing perpetrators’ use of violence.
Who has a role in the service system?
Family violence risk assessment and management is a shared responsibility across Victoria’s service system.
As the final report of the Royal Commission states:
Broadening responsibility for addressing family violence will require each sector or component part of the system to reinforce the work of others, collaborate with and trust others, to understand the experience of family violence in all its forms.[5]
Professionals from a broad range of services, organisations, professions and sectors have a shared responsibility for identifying, assessing and managing family violence risk, even where it may not be core business.
Together, they form the family violence service system, and are formally recognised and prescribed by regulation as ‘framework organisations’. The full list of framework organisations is available online.
Many professionals who have not traditionally had a role in assessing and managing family violence risk with victim survivors or perpetrators will now need to be familiar with these processes.
You are not expected to become a family violence expert – but everyone has a role.
This will vary based on the nature of your organisation and the type of contact you have with people experiencing and using family violence.
The MARAM Framework and Practice Guides are designed to help professionals in the service system, spanning specialist family violence services, community services, health, justice and education, to work together in responding to family violence, supporting victim survivors to be safe and recover from violence, and keeping perpetrators in view and held to account.
Given the prevalence of family violence, it is likely that most professionals and services across the community will come into contact with people experiencing and using family violence.
Any organisations not prescribed as ‘framework organisations’ can be guided by the MARAM Framework to identify how adult and child victim survivors can be better supported to disclose, be safe and recover from family violence, and to engage with perpetrators to invite personal accountability for their use of violence and motivate them to change.
While non-prescribed organisations and professionals are not required under the FVPA to align their policies, procedures, practice guidance and tools with the MARAM Framework, they are encouraged to do so.
This includes understanding the MARAM Framework and its application to their service users and incorporating relevant guidance on foundation knowledge and responsibilities into their work.
You may find the MARAM Framework and the Practice Guides can improve your response to family violence and assist with intervening earlier and connecting service users to the family violence service system.
6.1 Working with perpetrators
Professionals across the service system have a role in keeping perpetrators engaged and in view of services, contributing to accountability for their use of family violence and supporting them to change their behaviour – whether directly or indirectly.
The Royal Commission identified opportunities for a broader range of professionals and sectors to play a role in the integrated family violence system and support identification, risk assessment and management of people who use violence.[6] Working with people using violence can support professionals and the service system to keep victim survivors safe from violence. Identifying, assessing and managing family violence risk are crucial elements of a broad robust approach to perpetrator accountability.
Your professional and sector role will determine your level of responsibility in relation to perpetrators, and guidance and tools are provided in the perpetrator-focused MARAM Practice Guide.
6.1.1 Increased risk arising from perpetrator interventions
Interventions with perpetrators may increase risk to adult and child victim survivors.
They may also increase a perpetrator’s risk to themselves (from suicide or self-harm) or to professionals/community (such as threats to harm). Call Triple Zero (000) in an emergency or if there is imminent risk.
You should understand the potential for certain interventions to adversely affect people using violence from Aboriginal communities based on their connection, or lack of connection, to community and culture.
Seek secondary consultation with specialist Aboriginal community organisations to inform your understanding of interventions and their possible unintended effects.
Refer to your service’s policies and procedures for working with service users both within agency environments and when conducting home visits or outreach activities.
If you have a role in also working with a victim survivor, consider if it is safe, appropriate and reasonable to contact them and share information about increased risk, or another service working with a victim survivor to respond to increased risk.
Plan your approach to assessment to support safe engagement.
You should also engage in reflective practice and supervision to explore both perceived and real risks to your own safety, including any fears you have of directly working with perpetrators.
In planning with your supervisor, determine required supports, ways to manage risks to yourself and the service user, and alternative arrangements, if appropriate, to support the engagement and monitoring of the person using violence.
Secondary consultation with specialists may support your safe engagement.
Share information with other engaged services to ensure support is provided for the victim survivor as needed, due to increased risk that may arise from some perpetrator interventions if not actively managed.
The Organisation Embedding Guidance and Resources contains more information on worker safety.
MARAM practice responsibilities for professionals
Pillar 3 of the MARAM Framework outlines 10 Responsibilities of practice for professionals working in organisations and sectors across the family violence service system.
Organisational leaders will support professionals and services to identify which victim-survivor and perpetrator-focused MARAM Practice Guides are relevant for their role and functions.
The Practice Guides have been developed for working directly with service users (victim survivors and/or perpetrators).
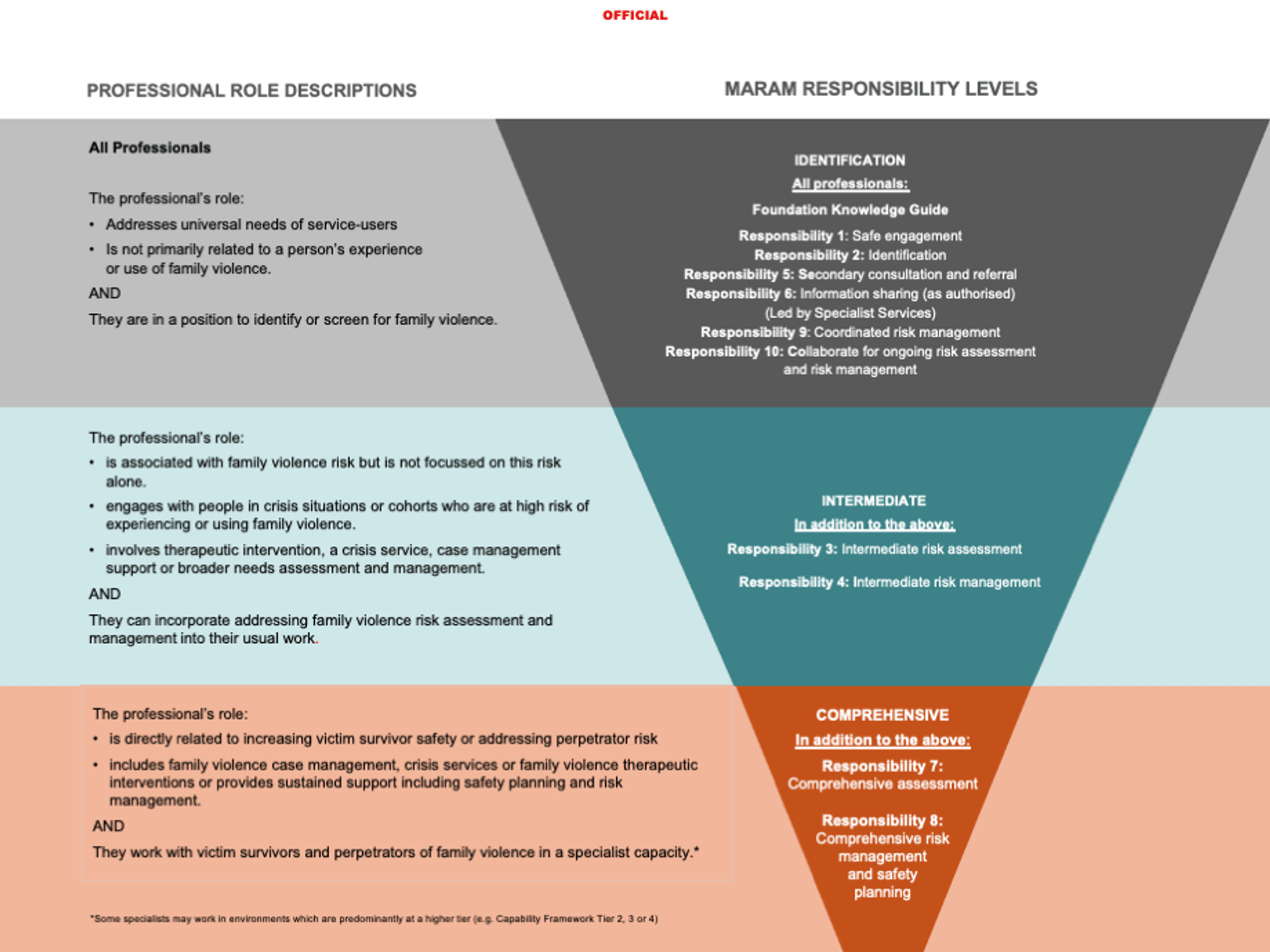
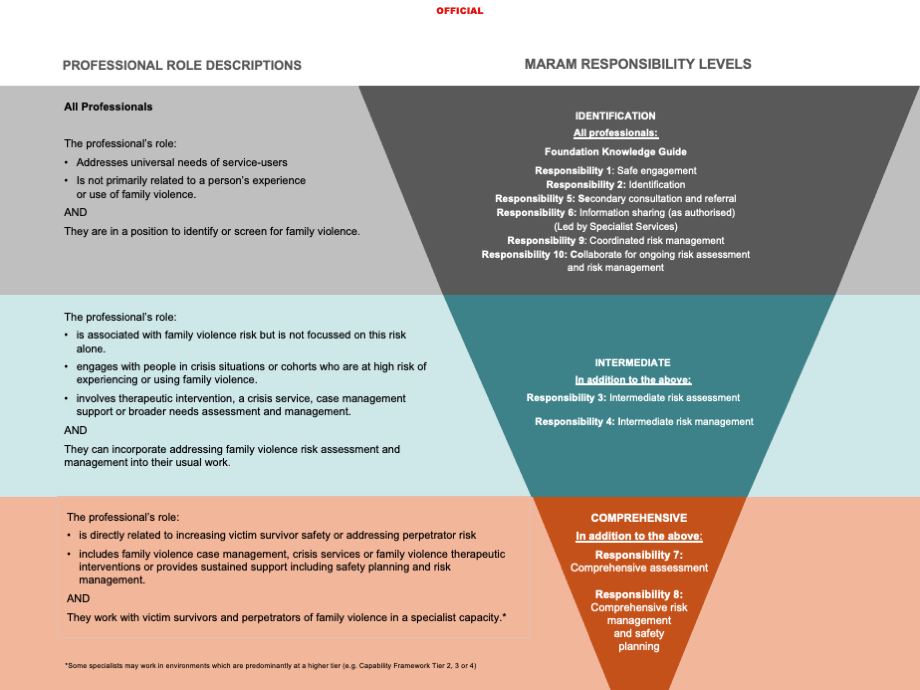
Responsibilities 1, 2, 5, 6, 9 and 10 as outlined below apply to all relevant professionals and services within prescribed organisations.
Some professionals also have a role in risk assessment and management at either the intermediate (Responsibilities 3 and 4) or comprehensive (Responsibilities 7 and 8) levels.
All organisational leaders in prescribed framework organisations are required to understand the roles and responsibilities of professionals and services within their organisation.
Identifying and mapping these roles within and across the organisation will support shared understanding of roles and responsibilities.
This will help professionals and services to work together to identify, assess and manage family violence risk through information sharing, secondary consultation and referral.
Remember
Professionals across a range of services and sectors have a role in working with victim survivors and/or perpetrators of family violence. The MARAM Practice Guides reflect what a professional should know to work with adult and child victim survivors, and adult perpetrators.
Table 1: Description of each practice responsibilities[7]
|
Risk assessment and management responsibilities |
Expectations of framework organisations and section 191 agencies |
|
Responsibility 1: Respectful, sensitive and safe engagement |
Ensure staff understand the nature and dynamics of family violence, facilitate an appropriate, accessible, culturally responsive environment for safe disclosure of information by victim survivor service users, and to respond to disclosures sensitively. Ensure staff recognise that any engagement of service users who may be a perpetrator must occur safely and not collude or respond to coercive behaviours. |
|
Responsibility 2: Identification of family violence |
Ensure staff use information gained through engagement with service users and other providers (and in some cases, through use of screening tools to aid identification/or routine screening of all service users) to identify indicators of family violence risk and potentially affected family members. Ensure staff recognise that any engagement with a service user who may be a perpetrator must also be culturally responsive and respond to coercive behaviours in a safe, non-collusive way. |
|
Responsibility 3: Intermediate risk assessment |
Ensure staff can competently and confidently conduct intermediate risk assessment of adult and child victim survivors using Structured Professional Judgement and appropriate tools, including the Brief and Intermediate Assessment tools. Where appropriate to the role and mandate of the organisation or service, and when safe to do so, ensure staff can competently and confidently contribute to risk assessment through engagement with a perpetrator, including using Structured Professional Judgement and the Intermediate Assessment, and contribute to keeping them in view and accountable for their actions and behaviours. |
|
Responsibility 4: Intermediate risk management |
Ensure staff actively address immediate risk and safety concerns relating to adult and child victim survivors, and undertake intermediate risk management, including safety planning. Those working directly with perpetrators attempt intermediate risk management when safe to do so, including safety planning. |
|
Responsibility 5: |
Ensure staff seek internal supervision and further consult with family violence specialists to collaborate on risk assessment and risk management for adult and child victim survivors and perpetrators, and make active referrals for comprehensive specialist responses, if appropriate. |
|
Responsibility 6: Contribute to information sharing with other services (as authorised by legislation) |
Ensure staff proactively share information relevant to the assessment and management of family violence risk and respond to requests to share information from other information sharing entities under the Family Violence Information Sharing Scheme, privacy law or other legislative authorisation. |
|
Responsibility 7: Comprehensive assessment |
Ensure staff in specialist family violence positions are trained to undertake Comprehensive assessment of risks, needs and protective factors for adult and children victim survivors. Ensure staff who specialise in working with perpetrators are trained and equipped to undertake Comprehensive risk and needs assessment to determine seriousness of risk of the perpetrator, tailored intervention and support options, and contribute to keeping them in view and accountable for their actions and behaviours. |
|
Responsibility 8: Comprehensive risk management and safety planning |
Ensure staff in specialist family violence positions are trained to undertake comprehensive risk management through development, monitoring and actioning of safety plans (including ongoing risk assessment), in partnership with the adult or child victim survivor and support agencies. Ensure staff who specialise in working with perpetrators are trained to undertake comprehensive risk management through development, monitoring and actioning of risk management plans (including information sharing); monitoring across the service system (including justice systems); and actions to hold perpetrators accountable for their actions. This can be through formal and informal system accountability mechanisms that support perpetrators’ personal accountability, to accept responsibility for their actions, and work at the behaviour change process. |
|
Responsibility 9: Contribute to coordinated risk management |
Ensure staff contribute to coordinated risk management, as part of integrated, multidisciplinary and multiagency approaches, including information sharing, referrals, action planning, coordination of responses and collaborative action acquittal. |
|
Responsibility 10: Collaborate for ongoing risk assessment and risk management |
Ensure staff are equipped to play an ongoing role in collaboratively monitoring, assessing and managing risk over time to identify changes in assessed level of risk and ensure risk management and safety plans are responsive to changed circumstances, including escalation. Ensure safety plans are enacted. |
The Organisation Embedding Guidance and Resources and the Responding to family violence capability framework provides information for organisational leaders on how to support their staff to identify the 10 Responsibilities that apply to their roles and services.
The relevant knowledge and skill indicators have been considered in the development of these MARAM Practice Guides for the MARAM Framework.
The MARAM Framework and Practice Guides should be interpreted to complement and build on existing practice frameworks, that will also continue to apply.
A high-level description of the MARAM Responsibilities and role descriptions are in Figure 2.
Figure 2: MARAM responsibilities and role descriptions
{kind=link}
7.1 How victim survivors or perpetrators access the service system
Victim survivors and perpetrators of family violence can access or interact with the family violence service system in a number of ways including:
Table 2: Entry points and services
|
Entry points |
Description of service types |
|
Specialist family violence and sexual assault services |
Specialist family violence services[8] such as crisis refuge services and services that specialise in working with Aboriginal communities, diverse communities and older people experiencing family violence or using family violence Multi-Disciplinary Centres and sexual assault support services |
|
The Orange Door |
Specialist family violence services for adult and child victim survivors, child and family services, adult perpetrator services |
|
Victim Support Agency |
Specialist family violence responses for adult male victims |
|
Prescribed justice and statutory bodies |
Police, courts, tribunals and correctional services, services for victims of crime, Child Protection and legal services[9] |
|
Prescribed universal services |
Education, social/public housing services, health services, maternal and child health services, state funded aged care services, mental health services, drug and alcohol services, disability services, financial counselling and community-based child and family services |
|
Targeted community services |
Services (in addition to community-specific specialist family violence services, above) with an expert knowledge of a particular diverse community and the responses required to address the unique needs and barriers faced by this group. Targeted services may also include community-specific services, such as ethno-specific, LGBTIQ and disability services that focus on primary prevention or early intervention. |
Having multiple entry points to the family violence service system means people can access the services they need and also be connected to appropriate support in relation to their experience or use of family violence.
A broad range of sectors and organisations serve as entry points for victim survivors and perpetrators[10] through risk identification, assessment and risk management, as appropriate to their role and the responsibilities embedded within their internal policy arrangements.
These sectors and organisations must also work with other services (such as specialist family violence services) to support coordinated and collaborative responses to family violence risk, such as sharing information to support risk assessment and management through secondary consultation.
About family violence
Family violence is behaviour that controls or dominates a family member and causes them to fear for their own or another person’s safety or wellbeing.
Family violence is behaviour that controls or dominates a family member and causes them to fear for their own or another person’s safety or wellbeing.
It includes exposing a child to these behaviours, as well as their effects and impacts. Family violence presents across a spectrum of risk, ranging from subtle exploitation of power imbalances, through to escalating patterns of abuse over time.
As described throughout this Foundation Knowledge Guide, family violence is deeply gendered. While people of all genders can be perpetrators or victim survivors of family violence, overwhelmingly, perpetrators are men, who largely perpetrate violence against women (who are their current or former partner) and children.
However, family violence can occur in a range of ways across different relationship types and communities, including but not limited to the following:
- children and young people as victim survivors in their own right who have unique experiences, vulnerabilities and needs
- older peoples’ experiences of family violence, often described as elder abuse, from intimate partners, adult children or carers, or extended family members
- varying experiences of family violence for people from Aboriginal communities may occur in intimate relationships, other family relationships, from people outside of the Aboriginal community who are in intimate relationships with Aboriginal people, and violence in extended families, kinship networks and community violence, or lateral violence, within the Aboriginal community (often between Aboriginal families).It extends to one-on-one fighting, abuse of Aboriginal community workers, as well as self-harm, injury and suicide[11]
- experiences of family violence for people from diverse communities, including in intimate relationships, extended family networks community violence and violence from a family of origin.
The FVPA provides a broad definition of family violence and ‘family’ or ‘family-like’ relationships, as outlined below. Family violence takes a variety of forms and occurs in a range of relationships, including and outside of intimate, domestic partners. The Preamble to the FVPA also notes a range of features of family violence and its significant effects on individuals, communities and families.
8.1 How the Act defines family violence
The FVPA defines family violence as behaviour by a person towards a family member or person that is:
- physically or sexually abusive
- emotionally or psychologically abusive
- economically abusive
- threatening
- coercive
- in any other way controls or dominates the family member and causes that family member to feel fear for the safety or wellbeing of that family member or another person.
It also includes behaviour by a person that causes a child to hear or witness, or otherwise be exposed to the effects of behaviour referred to in these ways.
Examples of family violence that are referred to in the Act (s. 5(2)) include:
- assaulting or causing personal injury to a family member, or threatening to do so
- sexually assaulting a family member or engaging in another form of sexually coercive behaviour, or threatening to engage in such behaviour
- intentionally damaging a family member’s property, or threatening to do so
- unlawfully depriving a family member of their liberty or threatening to do so
- causing or threatening to cause the death of, or injury to, an animal, whether or not the animal belongs to the family member to whom the behaviour is directed, so as to control, dominate or coerce the family member.
Coercive control
Coercive control is recognised within the FVPA, where family violence is framed as ‘patterns of abuse over a period of time’, inclusive of behaviours that coerce, control and dominate family members.[12] Coercive control is central to the definition of family violence within Victoria and understanding of risk identification and assessment.
Coercive control is not a standalone form of family violence. The term reflects the pattern and underlying feature or dynamic created by a perpetrator’s tactics and use of family violence and its felt impact or outcome on victim survivors.[13] As a tactic, coercive control can include any combination of family violence behaviours (risk factors) used by a perpetrator to create a pattern or ‘system of behaviours’ intended to harm, punish, frighten, dominate, isolate, degrade, monitor or stalk,[14] regulate and subordinate the victim survivor.
Coercive controlling behaviours may or may not include physical or sexual assault or threats to kill the adult or child victim survivor. However, the use or threat of these behaviours, even once, can create significant, ongoing threat of reoccurrence, creating and reinforcing an environment of coercive control.
The power and control dynamics underpinning family violence can have significant cumulative psychological, spiritual and cultural, physical and financial impacts on victim survivors. This can undermine a victim’s autonomy, capacity for resistance and sense of identity and self-worth.[15] A victim survivor can feel trapped within their experience of coercive control, where their options for accessing safety and support are removed, restricted or regulated.
High levels of coercive control are an indicator for increased likelihood of adult or child victim survivor/s being killed or seriously injured.[16]
Recognising patterns of behaviour that underpin coercive control can enable broader recognition of family violence outside of overt or discrete ‘incidents’ of physical and sexual violence.
Recognised forms of family violence under the FVPA are continuously evolving as the evidence base on presentations of risk across communities is strengthened. This guide seeks to provide information on presentations of risk for individuals and families across the community and will be updated as the evidence base for practice evolves.
Family violence can occur in relationships between spouses, domestic or other current or former intimate partner relationships,[18] in other relationships such as parent/carer–child, child–parent/carer, siblings and other relatives, including between adult–adult, extended family members and in-laws, kinship networks and in family-like or carer relationships. There may be more than one person using or experiencing family violence in the family, in a range of different relationship types.
The FVPA uses a broad definition of ‘family’ and ‘family-like’ relationships, covering:
- a person who is, or has been, the relevant person’s spouse or domestic partner
- a person who is, or has had, an intimate personal relationship with the relevant person
- a person who is, or has been, a relative of the relevant person
- a child who normally or regularly resides with the relevant person or has previously resided with the relevant person on a normal or regular basis
- a child of a person who has, or has had, an intimate personal relationship with the relevant person
- any other person whom the relevant person regards or regarded as being like a family member (for example, a carer).
Determining whether a person is a family member must consider relationships in their entirety. Section 8 of the FVPA provides some guidance on how to determine this.
Aboriginal communities define family violence to include a range of physical, emotional, sexual, social, spiritual, cultural, psychological and economic abuses that occur within families, intimate relationships, extended families, kinship networks and communities. It extends to one-on-one fighting, abuse of Indigenous community workers as well as self-harm, injury and suicide.[19]
The Dhelk Dja definition of family violence acknowledges the impact of violence by non-Aboriginal people against Aboriginal partners, children, young people and extended family on spiritual and cultural rights, which manifests as exclusion or isolation from Aboriginal culture and/or community.[20]
Family violence against Aboriginal people also needs to be understood in the context of structural inequality, barriers and past and present discrimination experienced by Aboriginal people, further outlined in Section 12.1.4, ‘Family violence against Aboriginal people and communities’.
8.2 Family violence that is a criminal offence
Family violence includes a continuum of behaviours, some of which are criminal offences.
Action can be taken against perpetrators for some acts of family violence that are criminal offences in their own right, such as stalking, physical assault, sexual assault, threats, pet abuse, property damage and theft.
Some risk factors that are recognised as family violence (both criminal and non-criminal behaviours) may be the subject of a family violence intervention order.
A breach[21] of an intervention order could also result in criminal charges.
In Victoria, family violence offences fall under two major categories:
- contravention of a family violence intervention order (FVIO) or a family violence safety notice
- criminal offences within a family violence context such as assault, property damage, stalking or threatening behaviour, sexual offences, theft and kidnapping or abduction.
8.3 Prevalence and drivers of family violence
Family violence is a deeply gendered issue rooted in structural inequalities and an imbalance of power between women and men.
The causes of family violence are complex. They include gender inequality and community attitudes towards women. Gender-based violence is violence that is specifically directed against women or that affects women disproportionately.
Gender-based violence is any form of violence targeting a person on the basis of their gender or gender presentation. It is recognised that gender-based violence disproportionality effects women.
In Victoria, family violence is the most pervasive form of violence perpetrated against women.
While people of all genders can be perpetrators or victim survivors of family violence, overwhelmingly, perpetrators are men, who largely perpetrate violence against women (who are their current or former partner) and children.
The majority of men who experience family violence are victim survivors of other male family members’ use of violence.
The 2021 National Homicide Monitoring Program report found women are over-represented as victims of intimate partner homicide.[22] On average, one woman each week is killed by a current or former male intimate partner, who in the overwhelming majority (92.6%) of cases was a primary perpetrator.[23] In comparison, one man each month is killed by a current or former intimate partner, and similarly the majority of men in these cases were the primary perpetrator (60.7%)[24] .
Women are also more likely to experience sexual violence from a current or former intimate partner.
Due to co-occurring structural inequalities, some women experience significantly higher levels of violence generally, including family violence.
Significantly, as outlined in the MARAM Framework, Aboriginal women are 32 times more likely than other women to be hospitalised and 10 times more likely to die from violent assault.
Women and girls with disabilities are twice as likely to experience violence as those without disabilities.
Children are victim survivors of family violence whether they are directly targeted by the person using violence or not. They may be subject to direct physical, sexual, psychological or emotional violence, or to threatening, coercive and controlling behaviours by a perpetrator.
Children and young people also experience family violence as victim survivors if they are exposed to the effects of a perpetrator’s violence towards any family member, even if they do not witness that violence directly.
The Royal Commission highlights that due to under-reporting of family violence and the lack of comprehensive data collection, it is difficult to assess the full extent to which children and young people experience family violence in Victoria. Children are often present or affected by family violence that occurs in the home.[25]
Where family violence is occurring in a family, there may be multiple perpetrators and/or victim survivors. In 2019–20, Victoria Police attended 88,214 family incidents, and children were recorded as present at 29.8% of these incidents where a parent/carer, was named as the affected family member.[26] In this time, period, children aged 17 years or younger were recorded as affected family members in 8.1$ of incidents.[27] The average age of children identified as affected family members or witnesses to family violence incidents was 12.4 years.[28]
In addition to gendered drivers, other drivers of family violence reflect structural inequality and discrimination. These include, but are not limited to, patriarchy, colonisation, racism, sexism, ableism, ageism, biphobia, homophobia and transphobia[29].
People from communities such as LGBTIQ communities, culturally, linguistically and faith-diverse and Aboriginal communities, may have a broad definition of family. This may include family of origin and family of choice, which can extend to close community members. The presentations of risk in each of these family relationships may be different.
In all these cases, family violence is characterised by ongoing patterns of coercive and controlling behaviours intended to create fear and/or compliance in victim survivors.
The drivers of family violence and family violence risk behaviours (risk factors) can occur across all relationship types and communities; however, they manifest in particular patterns within and towards Aboriginal communities, diverse communities and at various stages across the lifespan.
Family violence behaviours are produced by a complex relationship between a perpetrator’s thoughts, emotional responses, social learning and cultural factors. These can be challenging to distinguish from one another.
None of these factors excuse the use of family violence.
The use of family violence is a choice for which the perpetrator is ultimately responsible.
In the context of the broader family violence system, it is important that people who use violence are held accountable for their behaviour through both legal sanctions and service responses that encourage safety, change and taking personal responsibility.
Further information about presentations of risk across communities is outlined in the community-specific sections of this Foundation Knowledge Guide in Section 12. This includes prevalence and impact on victim survivors across age groups, Aboriginal communities, diverse communities and older people, and it outlines the behaviour and use of family violence by perpetrators in these communities.
Key concepts for practice
This section includes discussion of the following practice concepts and their relevance to victim survivor–centred practice.
They are:
- Structured Professional Judgement
- person-centred approaches
- intersectional approaches
- trauma and violence–informed approaches
- safe, non-collusive practice
- reflective practice and unconscious bias
- risk management approaches.
Each practice concept in this section can be applied to working with both victim survivors and perpetrators of family violence.
However, when working with perpetrators, you should maintain a focus on the experience of victim survivors and the impact of violence caused by the person using violence.
You can do this by remembering:
- to hold the victim survivor’s experience and safety at the centre of your assessment when engaging directly with the perpetrator
- perpetrators target aspects of a victim survivor’s identity, circumstances and experiences as part of their tactics and pattern of behaviour used to coerce and control them
- each perpetrator has their own identity, circumstances and experiences that affect their choice to use violence, the risk they present to family members, and their engagement with your service.
Information contained throughout the remainder of this Foundation Knowledge Guide will vary in language from the general ‘professionals’ to the specific ‘you’.
This information applies to all professionals, and you should consider the information as addressing you when either term is used.
10.1 Structured Professional Judgement
Using the practice model of Structured Professional Judgement allows you to assess information and determine the level or seriousness of risk to the victim survivor.
As a professional, you bring your experience, skills and knowledge to the risk assessment process to make an assessment.
10.1.1 Applying Structured Professional Judgement
When working with victim survivors, risk assessment relies on you or another professional ascertaining:
- a victim survivor’s self-assessment of their level of risk, fear and safety
- the evidence-based risk factors that are present.
You can gather information to inform this approach from a variety of sources, including:
- interviewing or ‘assessing’ the victim survivor directly or, where it is your role to do so, observing or assessing the perpetrator’s narratives, behaviours and their individual context and circumstances
- reviewing any information held by your organisation about the victim survivor or perpetrator
- requesting or sharing information, as authorised under applicable legislative Information Sharing Schemes, with other organisations about the risk factors present or other family violence risk-relevant information about a victim or perpetrator’s circumstances.
You should consider this information and apply your professional judgement to each of the elements. This is the act of you analysing and interpreting information to determine the level of risk.
Figure 3: Model of Structured Professional Judgement
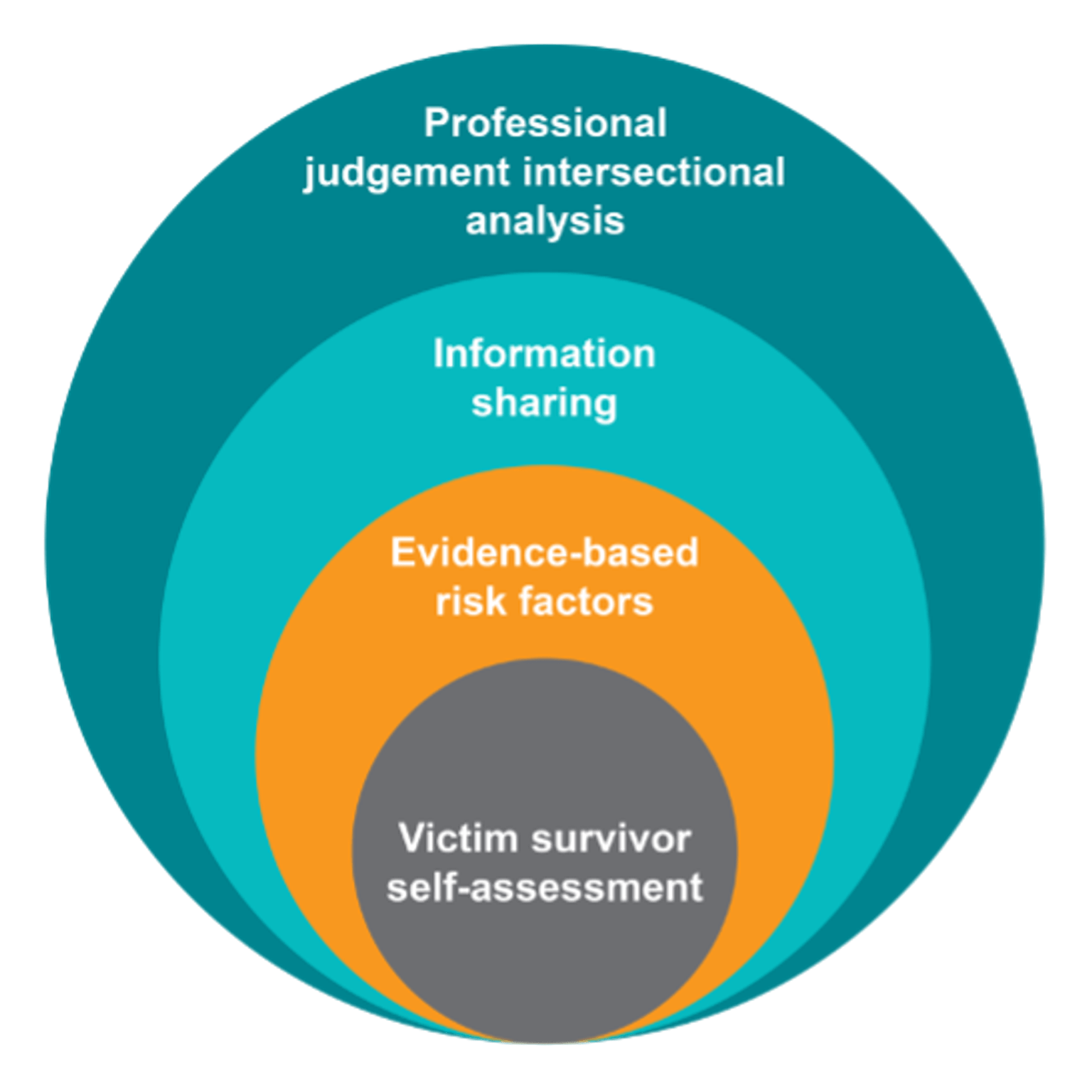
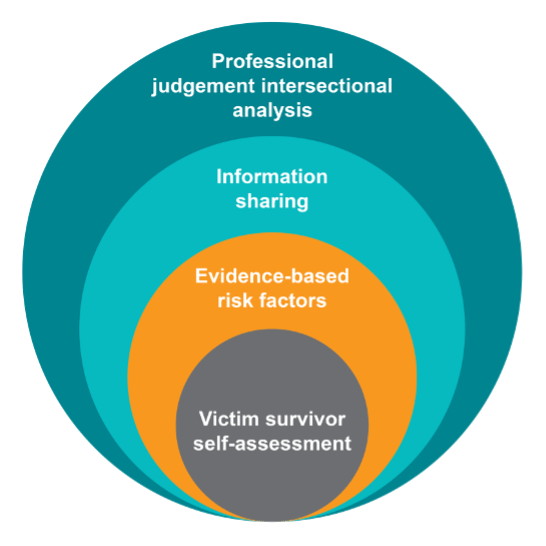{kind=link}
Assessing risk
Risk assessment is a point-in-time assessment of the level of risk. Risk is dynamic and can change over time. This means you should regularly review risk, and any changes should inform future assessment and risk management.
Your assessment of the level of risk, as well as appropriate risk management actions and approaches, must be informed by an intersectional analysis.
You should also consider relevant information about a victim survivor or perpetrator’s circumstances.
Best-practice approaches to risk assessment with a victim survivor enables them to share their story with you by you believing them about:
- their experience of violence
- the relationship
- how this has affected any children in the family (that is, understanding the risk experienced by children as victim survivors in their own right, which may also be informed by direct assessment of children)
- patterns of beliefs, attitudes, beliefs and behaviours of the perpetrator.
Evidence shows that adult victim survivors are often good predictors of their own level of safety and risk, and that this is the most accurate assessment of their level of risk.
By taking a person or victim-centred approach to risk assessment and management – listening to, partnering with and believing the victim survivor – you can recognise the victim survivor as experts in their own safety, with intimate knowledge of their lived experience of violence.
Sections 10.2 provides further detail on a victim-centred approach and applying an intersectional lens to family violence risk assessment and risk management.
10.1.2 Using Structured Professional Judgement with perpetrators
When you use Structured Professional Judgement when working with perpetrators, you must continue to centre the experience of the adult or child victim survivor. This is the case even when you do not work directly with the victim survivor to hear their own assessment of their level of risk.
When working directly with perpetrators, the practice of Structured Professional Judgement requires the following:
- Always centre the lived experience and risk to the victim survivor during your assessment by:
- observing behaviours or narratives disclosing family violence towards the adult or child victim survivors, and about the recent/current situation
- identifying overt and subtle violence-supporting narratives that indicate the person’s beliefs and attitudes about rigid gender roles, entitlement, power and control in relationships, expectations about women and partners (generally), and children and service involvement
- using your understanding of the impact of family violence in relation to any risk-relevant information disclosed or identified family violence behaviours. Remember that perpetrators will selectively disclose, if at all. They may disclose by way of seeking you to collude with their minimising, justifying or denying responsibility for their actions or behaviours
- seeking information from other services[35] to ascertain the victim survivors’ self-assessment of risk to inform your assessment. Where this is not possible, you will need to rely on your understanding of the impacts of family violence to inform your assessment.
- Identify the evidence-based risk factors present – it is likely risk is higher than indicated by any disclosure by the perpetrator or observed signs and narratives.
- Request or share information, as authorised, about the risk factors present, observations and signs, or other relevant information about a perpetrator’s risk and presenting needs and circumstances, to enable effective risk assessment and management.
- Apply intersectional analysis and your professional judgement throughout your assessment by:
- identifying if a perpetrator’s use of violence is patterned and targeting coercive controlling behaviours towards a victim’s identity or lived experience
- assessing, reflecting and seeking to understand the perpetrator’s presentation and narrative in the context of their own identity and lived experience
- identifying if there are structural inequalities or barriers to the perpetrator’s engagement with you, and whether they can name, disclose or understand what constitutes violent behaviours.
Structured Professional Judgement: what’s new?
The practice model of Structured Professional Judgement in the CRAF included victim survivor self-assessment, evidence-based risk factors and professional judgement. The MARAM Framework builds on this model and incorporates the new elements of information sharing and intersectional analysis. The model is applied when working directly with both victim survivors and perpetrators of violence.
10.2 Person-centred approaches
Using a person-centred approach can help you understand the profound impact violence has on adult and child victim survivors.
This approach gives the person space to describe the violence they have experienced, allowing you to sensitively identify presenting and cumulative risk and trauma.
As well as understanding their experience of family violence, you should also identify other factors in the victim survivor’s life that may create barriers or increased risk.
A person-centred approach combines intersectional analysis and trauma-informed practice, allowing you to:
- validate experiences of violence and its ongoing impacts
- be aware of the person’s experience of barriers, structural inequality and discrimination that may be co-occurring, which may also cause or exacerbate existing trauma.
You will then be able to tailor your responses to empower victim survivors to make informed choices and access services and supports they need.
10.2.1 Person-centred approaches with victim survivors
Your approach to engaging with victim survivors (adults and children) should be informed by the:
- person’s experience of family violence
- impact of the perpetrator’s violence on victim survivors’ daily functioning and relationships
- presence of any serious threat/risk
- person’s description of their relationship with the perpetrator
- person’s relationship with other family members (who might also be victim survivors or using violence), as well as other significant family relationships.
Remember that victim survivors will have a variety of views regarding their experience of violence from the perpetrator, as well as their own risk, safety and support needs.
They may also feel ashamed or afraid to disclose their experiences of violence. Their views may change over the course of your engagement and assessment with them.
Your support and assessment should align with the victim survivor’s own assessment of their risk, safety and support needs, where possible.
However, there may be times when, as a professional, you need to take action that does not align with a victim survivor’s views and wishes regarding support and interventions.
In some cases, different family members may assess their risk to be at different levels.
An adult victim survivor may minimise risk if they are afraid the perpetrator may use further violence following an intervention, or that a child may be removed from the home. Similarly, a child or young person may also hold views and wishes that cannot be acted on for legal or safety reasons.
In all cases, it is important to be transparent, where safe, appropriate and reasonable, with both adult and child victim survivors about the decisions you make and actions you take in relation to family violence risk and safety.
For all victim survivors, approaches should respond to a person's abilities and capacity to communicate so that they can make informed choices and provide input into the risk assessment and management process.
This is especially important when your professional or service response goes against the views and wishes of the victim survivor.
Using a person-centred approach means providing adequate, transparent information to victim survivors.
For children and young people, this should be appropriate to their age and developmental stage.
Before undertaking a risk assessment, you should give all service users information about your information sharing authorisation, discussed in the victim survivor and perpetrator-focused Responsibility 6.
When working with perpetrators you are not required to provide them with information that could increase risk to adult or child victim survivors.
10.2.2 Using a ‘person in their context’ approach with perpetrators
The key concepts of practice (person-centred, trauma-informed and intersectional analysis) are also relevant to working with people using family violence. However, when applying these approaches to working with perpetrators, it is essential to maintain a victim-centred lens.
Many aspects of a person-centred approach are applicable to working perpetrators of family violence. Developing trust and rapport is critical to maintaining engagement with perpetrators, to respond to their presenting needs and circumstances and address their use of violence.
However, throughout your engagement, you must maintain a victim-centred lens and prioritise the views, needs and safety of victim survivors.
A ‘person in their context’ approach uses aspects of person-centred practice with perpetrators.
It identifies and takes into consideration the perpetrator’s presenting needs, history and experiences, risks, strengths and environmental contexts or circumstances. It helps to build an understanding of the person’s life experiences that inform their interactions and relationships with friends, family, community, services and society. This includes the values, norms and beliefs that shape their views and expectations. These are expressed in their narratives about their role and relationships, likelihood of continued violence and/or escalation over time, and barriers to personal accountability, safety and change.
In this way, considering the ‘person in their context’ can include the:
- person’s experience of family violence as a child, in other family or previous relationships
- person’s use of violence in previous relationships
- impact of their use of violence on victim survivors’ and their own daily functioning and relationships, including their parenting role
- presence of any serious threat/risk to the victim survivor, themselves or another person
- person’s description of their relationship with the victim survivor
- person’s relationship with other family members (who might also be victim survivors or using violence), as well as other significant family relationships
- person’s relationship with social, cultural and community networks
- presence of and relationship with professionals, services and systems
- any environmental factors that impact on their life.
Situating the ‘person in their context’ is an important starting point for your engagement with people you know or suspect are using family violence.
This includes developing an awareness and understanding of the:
- multiple ways that power is used and experienced within personal, family, community relationships and society broadly
- dynamics associated with the service user’s behaviour towards others
- issues affecting their circumstances, health, wellbeing and needs
- protective or stabilising factors that minimise likelihood of harm to self and risk to others.
Remember that people who use family violence are not a homogenous group.
They will have a range of identities and variety of lived experiences that have shaped their historical and current behaviours, impact on their level of risk, and influence their capacity and willingness to change.
This contextual information informs your professional judgement, assists you to identify the person’s needs, as well as those of adult and child victim survivors, and contributes to risk management activities.
10.3 Intersectional approaches
Both victim survivors and perpetrators of family violence may experience intersecting forms of power and privilege, or discrimination and disadvantage.
Intersectionality, or intersectional analysis, is a theoretical approach recognising the interconnected nature of social categorisations and identities with experiences of structural oppression, discrimination and disadvantage. [36]
The theory of intersectionality can help you to understand and examine power, privilege and oppression, and how these overlap or intersect in people’s lives to reinforce and produce power hierarchies.
Many people’s experience is shaped by multiple identities, circumstances or situations. Applying an intersectional lens means considering a person’s whole, multi-layered identity and life experience to understand the ways in which they have, and may continue to, experience inequality and oppression.[37]
This can shape a person’s experience of the impact of family violence, the nature of a perpetrator’s violent and controlling behaviours and access to services.
For example, if an Aboriginal person also identifies that they have a disability, you should respond in your risk assessment and management practice to address any combined associated barriers. This provides a respectful, safe and tailored approach (also refer to the victim survivor and perpetrator-focused Responsibility 1).
In this guide, intersectional analysis reflects an individual’s age, gender identity, sexual orientation, ethnicity, cultural background, language, religion, visa status, class, socioeconomic status, ability (including physical, neurological, cognitive, sensory, intellectual or psychosocial impairment and/or disability) or geographic location.
Gender and the drivers of family violence are critical to informing your understanding of intersectional analysis in the family violence practice context.
Structural inequality and discrimination create and amplify barriers and risk, which continue to exacerbate systemic marginalisation, power imbalance and social inequality.
Your organisation’s policies, practices and procedures can either address these inequalities, or contribute to them further by privileging the dominant group and reinforcing the exclusion of people outside of it.
People and communities experience structural inequality, barriers and discrimination as oppression and domination. These relate to the impacts of patriarchy, colonisation and dispossession, racism, ableism, ageism, biphobia, homophobia and transphobia.
When applying an intersectional lens, you must reflect on and understand your own bias, so you can respond safely and appropriately in practice. You can use supervision with managers and engagement with colleagues to reflect on and respond to bias.
The MARAM Practice Guides provide extensive information about applying an intersectional analysis lens to working with both victim survivors and perpetrators.
10.3.1 Applying an intersectional lens
Experiences of structural inequality, barriers or discrimination can alter the way family violence is:
- experienced by individual victim survivors who identify as belonging to a community or communities
- perpetrated by people using violence who identify as belonging to a community, or from perpetrators outside of the community who are using violence against an individual who identifies as belonging to a community.
Using an intersectional approach with victim survivors
In many instances, these factors contribute to increased risk and amplify barriers to disclosure, service access and engagement.
Applying an intersectional analysis lens allows you to explore the impacts of systemic and interpersonal discrimination and disadvantage on marginalised groups.
This can influence how victim survivors:
- talk about, recognise and understand their experience of family violence by the perpetrator
- understand their options or decisions about what services to access based on actual or perceived barriers. This may be due to past discrimination or inadequate service responses from the service system, including from institutional or statutory services
- describe and/or are differently impacted by their experience of family violence by the perpetrator, and violence generally.
You should reflect on your own practice and biases in considering how Aboriginal people or people from culturally diverse communities or at-risk age groups may experience barriers, discrimination and inequality.
You should also consider where you can improve and tailor your practice approach to:
- improve people’s access to resources or services, such as support to respond to family violence risk
- increase the social and economic power service users hold
- counteract the perceived negative self-worth and marginalisation of some groups, which may increase the probability of violence being used against them.
Using an intersectional approach with perpetrators
Intersectional analysis can also help you understand perpetrators’ uses of violence against child and adult victim survivors, including how they:
- engage with the service system and seek help – based on actual or perceived barriers due to discrimination, inadequate service responses, negative beliefs about help-seeking (often associated with masculine identity)
- disclose and talk about their use of family violence – including how they understand, minimise, justify, or rationalise their use of violence
- engage in personal accountability and change – for example, motivations to change and perceptions of how accountability may present in particular ways for people from Aboriginal and diverse communities. This may be due to their particular identity, experience and place in relation to the community
- become ready or motivated to change, given any complex needs as well as internal and external motivators or barriers.
10.3.2 Professional reflection
To address potential barriers, person-centred practice uses an intersectional lens and adopts culturally sensitive and safe practices when undertaking risk assessment and management.
Professionals can also collaborate with organisations that specialise in supporting communities, to provide responsive and appropriate services (also refer to Responsibilities 5 and 6).
All family violence involves a perpetrator using patterns of coercive and controlling behaviours against one or more victim survivors.
Patterns of family violence behaviours can be recognised as manifesting in particular targeted ways when used against Aboriginal people, those from diverse communities and children, young people and older people.
The identities and experiences of both the victim survivor/s and the perpetrator inform the perpetrator’s choices to use coercive, controlling and violent behaviour.
These behaviours often target the identity or perceived ‘vulnerability’ of the victim survivor. This includes exploiting the victim survivor’s experience of structural inequality, barriers or discrimination.
For example, victim survivors who are Aboriginal or belong to a diverse community or at-risk age group, such as children, young people and older people, may be reluctant to report or engage with professionals or services about their experience of violence.
Aboriginal people may be reluctant to engage because services are not, or have not been, accessible, safe or responsive to their needs.
In particular, Aboriginal women or women from diverse communities are affected by multiple barriers, structural inequalities and discrimination. Their experiences of violence have historically been dismissed, minimised or ignored.
This means they have real and perceived barriers to engagement. These experiences can also lead to trauma, affecting an individual’s presentation, needs and ability to engage with services in different ways.
People who use family violence can concurrently experience power and privilege, and disadvantage and marginalisation.
Intersectional analysis allows us to understand that some people enjoy greater privileges than others.
For example, white, heterosexual, able-bodied, cisgender men typically enjoy greater social, political and economic status than people who do not reflect these characteristics.
Many people who use family violence benefit from the effects of patriarchy, colonisation and dispossession, racism, ableism, ageism, biphobia, homophobia and transphobia.
They may choose to enact oppressive structures of power and control in their own families, while also experiencing oppression and powerlessness in other contexts.
Men who do not hold some of those attributes may still be privileged over women by virtue of their gender but may feel or experience being subordinate to the dominant masculine ‘ideal’ because of their race, religion, ethnicity, citizenship status or ability.
Research has documented the ways in which men from diverse communities have been stereotyped to create a hierarchy of masculinity.
For example, on a spectrum, some groups of men are consistently ‘feminised’, including gay-identifying men, men with disabilities, some men of Asian heritage and/or appearance, while working class and men of African descent have been represented as ‘too masculine’ or too overtly physical (while still being marginalised).[38]
This can play out in the forms of community and family violence they may experience (predominantly) from other men, and in their experience of structural inequality, barriers and discrimination in the community more broadly.
It is the responsibility of professionals and services to reduce and remove structural inequalities and barriers to engagement, not the responsibility of the service user.
You should also recognise the collective strengths and the social, cultural and historic contexts of Aboriginal people and people from diverse communities.
The concept of intersectionality informs much of this Foundation Knowledge Guide and both the victim survivor and perpetrator-focused MARAM Practice Guides.
In particular, Section 12, ‘Presentations of family violence in different relationships and communities’ considers each community using this intersectional lens.
10.4 Trauma and violence–informed practice
Trauma is defined as the experience and effects of overwhelming stress that result in a reduced ability to cope or integrate ideas or emotions that are the result of that experience.[39]
Trauma arises from activation of instinctive survival response to threats.[40]
It can occur through everyday events outside a person’s control (loss of housing or employment), exposure to vicarious trauma, collective trauma (such as large-scale emergencies, natural disasters, war, acts of terror), systemic violence (including institutions), interpersonal violence, neglect and abuse during childhood or adulthood (such as from an intimate partner, caregiver or known person/family member and stranger violence), and historical and intergenerational trauma.[41]
Complex trauma can result from repetitive, prolonged and cumulative violence. Complex trauma is often interpersonal, intentional, extreme, ongoing and can be particularly damaging when it occurs in childhood.[42]
Trauma for children may be identified as adverse childhood experiences, which typically include physical, sexual and emotional abuse, physical and emotional neglect or witnessing family violence as a child.[43]
Trauma and violence–informed practice considers ‘the intersecting impacts of systemic and interpersonal violence and structural inequities on a person’s life’.[44]
This includes using intersectional analysis to highlight current and historical experiences of violence so that symptoms are not understood as exclusively originating within the person. Instead, these aspects of their life experience are viewed as adaptations and predictable consequences of trauma and violence.[45]
10.4.1 Impacts of family violence trauma on victim survivors
Having a trauma-informed lens is essential when engaging in family violence risk assessment and management when working with victim survivors.
Key practice considerations include the following:
- Everyone experiences some level of trauma from family violence.
- Trauma affects each person differently.
Trauma and violence–informed services do not necessarily treat trauma, but instead work to ensure the service experience will not cause further trauma, harm or distress.
This includes providing safe environments for disclosure and understanding the effects of trauma. It also includes being able to recognise ‘symptoms’ and problems as coping mechanisms that may have initially been protective.[46]
Coping mechanisms may be resourceful and creative attempts to ‘survive adversity and overwhelming circumstances’.[47]
At all times, view behaviour as an adaptive response to challenging life experiences. All your interactions with service users should be respectful, empathic, non-judgemental and convey optimism.[48]
In the context of victim survivors’ experiences of family violence from a perpetrator, trauma can result from physical, emotional, psychological, spiritual and sexual abuse, neglect and witnessing of violence or its impacts.
It can result from a one-off event, a series of or enduring events, or from intergenerational trauma resulting from the impacts of violence or abuse in a family or community.
Trauma is inherent to victim survivors’ experience of family violence.
It is the result of events outside of a victim survivor's control. These events may be unexpected, and the person may be unable to stop them, as they have no control over the perpetrator’s choice to use violence.
It is not the event that determines if trauma will occur, but rather the person’s experience of it and the meaning they make of it.
This can also be shaped by a person’s developmental age and stage, their cultural or personal beliefs and/or the support available to them.[49]
The impact of these events is to display power differentials that position the person as powerless.[50]
Effects of trauma
The effects of trauma may be felt immediately or occur later in life.
The way trauma manifests for a victim survivor depends on a range of factors, such as the relationship with the perpetrator and whether they are believed and supported by family/friends or professionals.
Trauma can affect a person’s relationships with parents or carers, siblings or other family members, friends and social networks, as well as their housing security, and engagement in education, employment and community.
It can interrupt and change a child or young person’s development, including brain development, and is (more) likely to have long-term effects.
The impact of trauma in adulthood can manifest in different ways, and it is likely to be compounded if the person experienced childhood trauma (due to cumulative effects).
The impact of trauma on older people can be wide-ranging and will depend on their previous trauma experiences and current supports.
Trauma can have significant impacts on a victim survivor’s identity and can create feelings of shame and/or powerlessness, which may result in negative coping behaviours or avoidance.
While different people react to trauma in different ways, for some it can have lasting adverse effects on their functioning and mental, physical, social, emotional or spiritual wellbeing. Cumulative effects can manifest in many ways over a person’s lifetime.
While the effects of trauma can subside for some victim survivors once they are safe (for example, once they leave a violent relationship), this may also be when acute trauma responses commence.
A person can be ‘triggered’ by seemingly everyday events, where a person’s stress responses are activated in response to thoughts, sense activation, experience or interpersonal dynamics.
This can be experienced as a re-living of the original situation, and the person can respond from that space.
Trauma and violence survivors can be misunderstood as ‘overreacting’, when in their experience they are reacting to the trauma of the past. Their response can be both emotional and most likely also physiological (‘flight-fight-freeze’).
Children and young people who have experienced trauma have a greater likelihood of presenting with a physiological impact as a result, given their rate of neurobiological development. A child or young person’s neurobiology can become patterned to respond as if a threat is imminent even when it is not.
10.4.2 Trauma and violence–informed practice when working with Aboriginal people and communities
The disproportionate impact of family violence on Aboriginal people is deeply rooted in the intergenerational traumas endured as a result of invasion and the violent dispossession of land, culture and children.[51]
Remember
There is a gendered element to family violence for Aboriginal people, but family violence also sits within the violence of colonisation and its ongoing legacy, including the displacement of men from their traditional roles and the forced removal of children.
The ongoing legacy of these events continues to have profound impacts, including trauma and grief on Aboriginal people individually, and as families and communities. Aboriginal children continue to be removed from their families at disproportionately high rates because of the enduring impacts of intergenerational trauma, which can increase the likelihood of exposure to family violence.[52]
When working with Aboriginal people experiencing or using violence, as part of your engagement it is particularly important that you hold an understanding of trauma, including intergenerational trauma and the person’s healing journey.
You should offer the choice to engage with Aboriginal services to ensure trauma-informed approaches and cultural safety. The principles of Nargneit Birrang– Aboriginal Holistic Healing Framework for Family Violence can also guide your response.[53]
10.4.3 Locating non–family violence related trauma in your practice (intersectionality)
People from any identity or community can have experiences of collective trauma not related to family violence.
Pre-migration trauma is a contributor to perpetration of family violence against women and children in migrant and refugee communities.[54]
People from migrant and refugee backgrounds may have experiences of political violence and trauma in their home countries that have ongoing personal consequences.
They may have histories of family violence pre-dating immigration experiences and the effects of childhood experiences of violence.
Similarly, research has identified an association between men experiencing trauma in their country of origin and later perpetration of family violence. Trauma includes imprisonment, torture and involvement in conflict as a combatant and, for men, this was associated with negative mental health impacts and violent behaviours.[55]
10.4.4 Establishing a trauma and violence–informed approach with all service users
You should be aware of the signs and impacts of trauma when assessing and managing family violence risk. This is described in practice guidance for the victim survivor and perpetrator-focused MARAM Practice Guides for Responsibility 1.
For professionals who do not have mental health expertise, identifying the presence of trauma can be difficult.
Symptoms such as hypervigilance, which is commonly linked to trauma, are also often present among service users who appear resistant.
Trauma and violence–informed practice in the context of family violence is not about treating trauma conditions or symptoms – this can be supported by referral for specialist supports where it is not a part of your role.
Instead, it is about being sensitive to the impacts of trauma and ongoing structural inequality.
Applying a trauma and violence–informed approach to your work means:
- understanding the person’s experience of trauma and structural inequalities
- responding to the impacts of both on individuals, families and communities, avoiding re-traumatisation, and maximise engagement with your service.
It is important to approach all engagement with victim survivors and perpetrators[56] of family violence with a trauma and violence–informed approach.
This means:
- providing space for individuals to feel physically and psychologically safe
- seeking to build trust with service users, and as much as possible provide transparent service delivery
- modelling respectful relationships
- engaging in strengths-based ways
- supporting service users to make pro-social, non-violent choices that increase safety
- working against stereotypes and biases by using the person in their context approach.
10.4.5 Using a trauma and violence-informed approach when working with perpetrators of family violence
For people who use family violence, the impacts of trauma can be complex. Engaging with them through a trauma and violence–informed lens does not mean validating or excusing their behaviour.
Many people who use family violence have histories of adverse childhood experiences, including violence within their family.
Some people who use violence may have also experienced traumatic or violent events. This includes past and current impacts of colonisation, refugee and/or migration experiences, institutional racism, discrimination and stigmatisation, lateral violence and natural disasters.
These experiences can have severe impacts, including on physical, relational and emotional functioning, issues of emotional regulation and cognitive functioning, and diagnosed or undiagnosed mental health issues.
In some circumstances, the person’s own continued use of violence can compound their trauma responses.
When working with perpetrators, identifying trauma is important in addressing their health and wellbeing needs.
This may lead to a reduction of risk behaviours or positively contribute to engagement with services. If you are not trained in responding to trauma, you may need to refer the person to mental health services.
It is tempting within professional and therapeutic frameworks to believe that addressing perpetrators’ past and ongoing trauma will lead to attitudinal and behavioural change.
However, to be trauma-informed when assessing perpetrator risk, you must hold in balance that:
- using violence against adult and child victim survivors is a choice
- trauma can be a contributing factor in the use, change or escalation of family violence by the perpetrator if they are not being supported to take responsibility for managing it
- if unaddressed, trauma can negatively impact a perpetrator’s capacity to engage in change work.[57]
10.5 Safe, non-collusive practice
The term ‘collusion’ refers to ways that an individual, agency or system might reinforce, excuse, minimise or deny a perpetrator’s violence towards family members and/or the extent or impact of that violence.
Invitations to collude occur when the perpetrator seeks out the professional to agree with, reinforce or affirm their narrative about their use of violence, the victim survivors or their situation.
When taken up by professionals, this practice colludes with the perpetrator’s attempts to avoid responsibility for their use of violence.
10.5.1 Recognising collusion
Collusion takes many forms. Professionals collude by demonstrating compliant collusion (agreement) or through oppositional confrontation (reprimand or arguing with them).
It can be expressed with gestures implying agreement, a sympathetic smile or a laugh at a sexist or demeaning joke.
It is there when all or partial blame is laid on a victim survivor and when a perpetrator’s excuses are accepted without question.
Collusion by professionals is often unintentional.
It arises from the long-standing subjugation of women and legitimisation of various forms of violence against women and children.
It can be conscious or unconscious, and it includes any action that has the effect of reinforcing the perpetrator’s violence-supportive narratives as well as their narratives about systems and services.
Perpetrators can intentionally invite professionals to collude in their narratives. This gives the narratives legitimacy, while allowing them to avoid thinking critically about their behaviour and its impact on others.
Professionals have a responsibility to recognise invitations to collude.
This includes recognising your own discomfort when hearing perpetrators’ narratives and knowing when and how to adjust your responses to maintain the person’s engagement while holding awareness of their use of violence.
10.5.2 Effects of collusion
The effects of collusion depend on the form it takes. It can:
- strengthen the violence-supportive narratives and justifications that a perpetrator uses to excuse their use of violence
- strengthen and/or reinforce the ways that a perpetrator minimises or denies responsibility for their behaviour, thereby making it less likely they will stop their use of violence
- allow a perpetrator to call on the authority of a professional (such as a counsellor) to shore up their own position. For example, saying to a victim, ‘My counsellor agrees with me that you need to …’
- reinforce a perpetrator’s position to take an oppositional or argumentative stance that gets in the way of them taking responsibility for their behaviour
- allow a perpetrator to use the service system against family members. For example, by conveying the message that the service system is taking the perpetrator’s side and therefore that the victim’s resistance is futile.
10.5.3 Avoiding collusion
You can actively avoid collusion with a perpetrator by doing the following:
- Be aware of the ways that perpetrators invite collusion and pre-plan for the engagement.
- Consider your role and level of responsibility to directly engage with perpetrators about their use of violence, being mindful of any potential to increase risk of harm to victim survivors.
- Do not interview or ask questions of a victim survivor in the presence of a potential perpetrator or adolescent who may be using family violence. Doing so may increase the risk to victim survivors, including children.
- Reflect on your own practice and adopt a balanced approach to engagement (further information is at Responsibility 3)
- Consider sharing information or seeking secondary consultation with a specialist family violence service that can:
- support the person you suspect is experiencing family violence
- offer expertise in assessing perpetrator risk
- safely communicate with a perpetrator and engage them with appropriate interventions and services.
If you believe a person may be using violence and/or seeking your collusion with their use of violence, apply the principles of reflective practice and consult with your colleagues or consult with a specialist family violence service.
Seek ongoing professional development and refinement of skills with support of supervisors, practice leaders and specialist family violence services.
Some professionals are uniquely positioned through their engagement with perpetrators in non-specialist family violence service settings to hold information and take responsibility to support risk assessment and management of perpetrators of violence. These professionals and services can support perpetrator accountability in a range of ways.
Section 12 has more information about common perpetrator narratives in different contexts and communities. The perpetrator-focused Responsibility 1 provides more information on safe, non-collusive communication and Responsibility 3 provides more information on how to recognise invitations to collude and professional stances in practice and adopt a balanced approach to engagement.
10.6 Reflective practice and unconscious bias
Remember
Responsibility for the use of violence rests solely with the perpetrator.
Victim survivors are not to be blamed, held responsible or placed at fault (directly or as part of structural responses) for a perpetrator’s choice to use violence.
This includes shifting responsibility and accountability for violence and its impacts on children towards perpetrators, and away from adult victims’/non-violent parents’ perceived ‘failures’, such as within the concept of ‘protective parenting’.
The safety and wellbeing of children must be prioritised.
The practice of ‘tilting to the perpetrator’ should be used to hold perpetrators accountable for their ‘failure to protect’ children through their use of violence.
Professionals should work with adult victims/non-violent parents, to enhance their safety, stabilisation and capacity to also enhance the safety of children.
All decisions and judgements we make are influenced by our existing knowledge, perceptions and biases. These develop through socialisation, education and learned associations between various personal attributes, identities and social categories.
Biases are learned ideas, opinions or stereotypes formed throughout an individual’s personal and professional life through our understanding of culture, family, attitudes, values and beliefs (including religious beliefs).
Bias can occur when this experience and understanding leads to assumptions about individual people or communities based on their circumstances, personal attributes, behaviour and background. This includes characteristics such as a person’s age, gender identity, sexual orientation, ability or disability, faith, language and cultural background.
All people have these biases. As a professional, you should recognise your own biases in your approach to Structured Professional Judgement. You may be conscious or unconscious of the biases you hold.
Part of using an intersectional lens means being self-aware and thinking about how your own characteristics have shaped and informed your identity, as well as the biases you hold.
You should also reflect on your place in the service system’s creation of structural privilege and power, and how conscious or unconscious bias might affect your responses to service users. You can use supervision with managers and engagement with colleagues to reflect on and respond to bias.
Bias might relate to understandings and misconceptions about the prevalence and forms of family violence.
For example, research has shown that there continues to be a decline in the number of Australians who understand that men are more likely than women to perpetrate domestic violence. [58]
It is critical that all professionals are aware of the personal values that underpin their practice.
This includes recognising biases, judgements and assumptions that may affect service users’ engagement with services and thus inadvertently increase risk.
Practising this will support you to become aware and unpack your unconscious biases.
10.6.1 Bias in risk assessment and risk management
In the context of family violence risk assessment and risk management practice, bias can cause you to make judgements and assumptions about a person’s particular experiences or use of family violence and their level of risk.
It can also create, or fail to address, existing barriers in your engagement with service users or their engagement with other services.
Examples include:
- making assumptions about the effects of a person’s disability, such as assuming that a person with a disability that affects their communication has a cognitive or intellectual disability or presuming a person with disability does not have ‘capacity’
- minimising the experience of violence or its impacts on people with disabilities or older people if they require care and support, such as colluding with narratives of ‘carer stress’ or failing to recognise impacts due to the victim survivor's lower communication capacity
- stereotyping people from LGBTIQ communities, including by mischaracterising their experiences based on heteronormative assumptions, minimising or colluding with ‘mutualising’ language[59] or not recognising forms of family violence in LGBTIQ communities and relationships due to the dominant recognition of heterosexual intimate partner violence
- making assumptions about the experience and acceptability of family violence for people from culturally, linguistically and faith-diverse communities
- making assumptions about an older person’s universal capacity due to their age or presenting state of dependence, and/or presence of medical conditions which impact cognition such as dementia.
You should engage in reflective practice by considering how your own cultural norms and practices might manifest as conscious and unconscious biases affecting your decisions, engagement with service users and approaches to Structured Professional Judgement.
Due to the nature of unconscious bias, you may be unaware of its effects. This reflective practice should be supplemented through discussion of these issues in supervision, with colleagues with greater expertise in these areas, and/or through collaboration with services with experience and expertise in working with the community or group in question.
10.6.2 Cultural responsiveness
Cultural responsiveness means being alert to your own or other professionals’ potential biases, privileges and cultural stereotyping.
It also means you have a responsibility to educate yourself about the culture of the people you work with.
Cultures are continually evolving, and each person lives culture in their own way.
In addition to self-education, always invite people to help you understand what is culturally significant to them, individually and in their relationships with other family members. This includes parenting practices if children or young people are present.
Secondary consultation or partnership with a bi-cultural worker can help you build this understanding.
Strive to be curious and open to how culture might interact with other factors that impact on adults, children and young people.
10.6.3 Professional responsibilities, unconscious and conscious bias when working with perpetrators
It is important to remember that the role of many professionals is to engage with perpetrators so that they are in view of the service system, which supports keeping victim survivors safe.
Part of a professional’s responsibility to perpetrator accountability is ensuring that any negative views you may have about the perpetrator does not influence your direct engagement.
Enacting negative views in practice may create oppositional or confrontational engagement, which can escalate both the risk to the victim survivor and increase the likelihood that the perpetrator will disengage from your service and/or the system whose responsibility it is to keep them in view.
Recognising conscious and unconscious bias is described in perpetrator-focused Responsibility 1. Reflecting on your own practice to identify balanced, oppositional confrontation and compliant collusive approaches is described in perpetrator-focused Responsibility 3.
10.7 Risk management
Risk management should focus on the safety of victim survivors and actions that keep perpetrators in view and hold them accountable for their behaviours.
This includes actions to assist with:
- risk management and safety planning with adult and child victim survivors, including being responsive to immediate risk when violence is occurring, and supporting them to stabilise, move forward and recover from the violence they have experienced
- risk management interventions directly designed to reduce or remove perpetrators’ risk, support them to stabilise their needs and circumstances that relate to risk behaviours, take responsibility for their use of violence and support their capacity to make choices to stop using violence
- coordinating and collaborating across services to share information and plan risk management actions to keep victim survivors safe and perpetrators in view and accountable.
All prescribed organisations have some role in risk management matched to their responsibilities under the MARAM Framework.
10.7.1 Risk management responses and actions
Risk management is the intervention required to prevent or reduce the likelihood of future risk and respond to impacts of family violence that has occurred.
Risk management responses should be person or victim-centred and trauma-informed in their development, to ensure they are holistic and respond to a victim survivor’s needs and can promote stabilisation and recovery.
All risk management is based on risk assessment. It responds to the level of risk caused by the perpetrator’s use of violence and coercive control, including patterns and forms of violence that may target a victim survivor’s identity or experience of structural inequality, barriers or discrimination.
Actions that comprise risk management often include information sharing, secondary consultation and/or referral, coordinated and collaborative practice, risk management planning of perpetrator responses and interventions, safety planning directly with victim survivors and perpetrators and ongoing case management.
Risk management strategies that target a perpetrator’s behaviour include responding to their presenting needs and circumstances, without collusion, and identifying, understanding and managing their pattern of family violence over time.
This can include direct intervention to lessen or prevent further violence from occurring, responding to:
- current risk behaviours with interventions to increase accountability, and
- presenting needs and circumstances related to escalation of risk by coordinating with a range of police, justice, specialist family violence (perpetrator and victim) services, and other interventions.
10.7.2 Safety planning
Safety planning is one part of risk management. It typically involves a plan developed by a professional in partnership with the victim survivor or perpetrator.
When working with victim survivors, safety planning aims to:
- help manage their own safety in the short to medium term
- build on what the victim survivor is already doing to resist control, manage the impacts of the perpetrator’s behaviour and other actions aimed at keeping themselves safe.
When working with perpetrators, safety planning aims to:
- encourage them to take responsibility for their needs and circumstances that relate to escalating family violence risk behaviours
- stop their use of coercive, controlling and violent behaviours against family members, including through de-escalation strategies
- promote self-initiating engagement with professional services when their circumstances change or use of risk behaviours escalates (risk to self (suicide or self-harm) or risk to victim survivors).
Safety planning strengthens key ‘protective factors’ that promote safety, stabilisation and recovery. These include factors such as intervention orders, housing stability and safety, health responses, support networks, financial resources and responding to wellbeing and needs.
Where possible, safety planning with a perpetrator must take into account any safety plans in place for victim survivors.
Safety planning often requires a collaborative approach and information sharing with services working with:
- adult victim survivors
- children and young people who are victim survivors. This includes:
- within an adult victim survivor’s safety plan, with responses to each child’s risk and needs, and
- older children who may have their own safety plan with their input, where safe, appropriate and reasonable. This helps them identify with whom and where they feel safe, whom they can talk to and what actions they can take (such as calling police)
- adult perpetrators – with professionals separately considering any safety plans for adult and child victim survivors in context
- other family members or carers (who are not using violence).
10.7.3 Information sharing as risk management
The victim-survivor and perpetrator-focused MARAM Practice Guides for Responsibilities 2, 4, 6 and8 provide guidance on risk management at different levels of practice (identification, intermediate and comprehensive).
This includes safety planning, information sharing, secondary consultation and referral, coordinated and collaborative practice.
This guidance also covers how to manage risk for both adult and child victim survivors, and adult perpetrators.
The risk management actions that a professional or service should take to reduce or prevent the family violence risk behaviours of a perpetrator will vary according to roles and responsibilities.
In addition to the above, this may include:
- providing consistent community-level information and messages that violence will not be tolerated or accepted
- recognising invitations to collude with a perpetrator’s minimising or victim-blaming narratives
- assisting victim survivors to report family violence that is a criminal offence to police
- contributing to the monitoring of a perpetrator’s use of violence and sharing information with relevant organisations
- being responsive to the perpetrator’s presenting needs and circumstances, without collusion, and supporting service responses that address issues linked to family violence risk behaviours
- contributing to collaborative multiagency actions that are designed to increase safety for the victim survivor, for example, planning appointment times that reduce the likelihood of the perpetrator being aware of actions the victim survivor is taking to leave the home or attend an appointment
- safety planning directly with the perpetrator.
10.7.4 Worker safety
Interventions with perpetrators may increase risk to victim survivors and others within the community, including professionals.
All professionals must be mindful of policies and procedures for working with vulnerable service users, both within agency buildings and when conducting home visits or outreach activities.
At all times, you should have opportunities in the workplace to engage in reflective practice and supervision to explore both perceived and real risks to your own safety.
In planning with your supervisor, determine opportunities for support for yourself, ways to manage risks to you and your service users, and alternative arrangements to support the engagement and monitoring of the person using violence.
Further information on worker safety is in Workplace Support Plan in the Organisation Embedding Guidance and Resources.
Gendered drivers of family violence in the context of prevalence and identity
Outlines the particular dynamics and forms of family violence experienced by individual victim survivors and communities, from people using violence who identify as belonging to, or who are outside of, that community.
11.1 Introduction
The guidance in this section outlines the particular dynamics and forms of family violence experienced by individual victim survivors and communities, from people using violence who identify as belonging to, or who are outside of, that community.
The MARAM Framework Principles recognise different forms and dynamics of family violence, across ages and communities. Drivers of family violence risk are consistent with the overarching drivers of violence against women and children including: condoning violence against women, men’s control of decision-making and limits to women’s independence in public and private life, rigid gender roles and stereotyped constructions of masculinity and femininity, and male peer relations that emphasise aggression and disrespect towards women.[60]
Central to this is an understanding about how gendered drivers of family violence, in context to social norms and culture, influence a perpetrator’s choice to target the victim survivor’s identity.
Perpetrators may use family violence to target victim survivors’ identity, circumstances and experiences. This can exacerbate adult and child victim survivors’ experiences of structural inequality, barriers and discrimination. As part of their pattern of behaviours and tactics of coercive control, this can also have significant impacts on the safety, autonomy, freedom and health of victim survivors.
Most commonly, family violence presents as violence from cisgender men from the white dominant culture, who predominantly target women and children.
However, dominant gendered drivers, social norms and culture also produce the societal conditions and attitudes that influence perpetrators’ use of family violence across relationship types, identities and communities.
These social and cultural norms are referred to as the drivers of family violence . Examples of these drivers include gender inequality, heteronormativity, cisnormativity, ableism, classism, racism and the ongoing impact of colonisation.
In your work with any victim survivor or person using violence, being attuned to their identity and experiences will assist you to understand these factors.
In practice, you should seek to understand:
- how the identity, needs, circumstances and experiences of people who use violence relate to their choice to use violence, the risk they present to intimate partners, children and other family members, and how they engage with your service
- how each perpetrator uses aspects of a victim survivor’s identity and experiences and exploits these real or perceived ‘vulnerabilities’ as tactics to coerce or control them, or in the forms of violence they use
- how social inequality impacts on access to both formal and informal justice and social support systems, and whether family, friends, community and services believe victim survivors to offer support, or collude with perpetrators.
11.1.1 Gendered drivers in the context of social conditions, norms and culture [61] (prevalence of men’s use of family violence)
It is gender, not cultural background, that drives men’s perpetration of violence against women and family members.[62]
Research shows that men’s attitudes towards women and gender equality are the strongest indicator of their use of aggressive and violent behaviour towards women.[63]
You should understand the prevalence and drivers of family violence and the experiences of victim survivors before you proactively engage with known or suspected perpetrators of family violence.
Focusing exclusively on a perpetrator’s culture makes ‘invisible the violence that emerges from the dominant “culture”’.[64]
In Australia, the dominant white culture inherently condones violence and reflects the structures of power and privilege created, perpetuated by and primarily that benefits white, ‘masculine’, heterosexual men.
This also informs the way structures of power that marginalise some men contribute to ongoing violence against women and children.[65]
In dominant white culture, the use of violence against women and children, predominantly by men, is often presented as a juxtaposition of positive descriptions of ‘a good bloke’ with the minimising of responsibility when he is ‘pushed too far’.
In contrast, family violence in non-dominant Australian cultures is framed by comparing ‘tradition’ and ‘modernity’, incorrectly assuming that non-white cultures are more tolerant of men’s violence against women than white cultures.[66]
Reflections of family violence prevalence often locate the perpetrator as someone ‘other’ or ‘evil’, and not someone who is or could be a member of any family or social network. This is inconsistent with the evidence on the prevalence of family violence in the community, which demonstrates that perpetrators are usually ‘ordinary’ people whose presentation and circumstances may also be ‘ordinary’.
The role of social norms
Social norms and contemporary expectations about ‘ways to be a man’ are interwoven with our broader cultural ways of life and the way our political and economic institutions operate. This is not to suggest that all men embrace these norms. However, all men are affected by norms and expectations about masculinity, and their performance is often measured against these by themselves and others.
Examples of identified masculine norms for men in Western societies include[67]:
|
|
These norms or expectations influence men differently. They create incentives, pressures and learned ‘acceptable’ or encouraged behaviour.
This has a bearing on men’s behaviour in certain contexts and with certain peer groups. For example, expectations of the way men relate to men and women differ in the workplace and the home, compared with what has been historically acceptable behaviour in sporting clubs or on a ‘boys’ night out’.
There may be contexts in which men feel more comfortable or socially safe to call out sexist or homophobic behaviour, based on what is socially acceptable and the extent to which that will be ‘policed’ by other men.
Community expectations about social norms relating to gender, sexuality, sexual identity, race, religion and disability are fluid and are evolving.
At the same time, these norms are deeply embedded in our social, economic, political and cultural narratives. They may go unperceived, as they are considered ‘normal’ due to their predominance in the culture in which we live.
Public discourse on acceptable behaviour may also be at odds with beliefs in action. For example, public messaging about the unacceptability of violence against women is at odds with the findings of national relationship surveys on beliefs and attitudes towards women and children.[68]
Social conditions, dominant culture and norms contributing to prevalence and use of family violence by perpetrators, is discussed across each identity and community group, below.
11.1.2 Coercion and control
The underlying intention or choice for perpetrators to use or threaten violence against family members is to attain and maintain power over family members. They do this through a pattern of coercive and controlling behaviour that serves to undermine, disempower or isolate victim survivors. The social conditions underpinning intention and choice to use of family violence is detailed in Responsibility 2.
The way a perpetrator uses family violence depends on the personal, social and structural aspects they perceive as available to them to exert control over family members.
These may vary and be compounded by attitudes and social norms that operate within the perpetrator’s or the victim’s community.
While the perpetrator’s behaviour and tactics may manifest in different ways due to these factors, they ultimately seek to exert and maintain power and control within a relationship.
Perpetrators may internalise and invoke social norms and attitudes to undermine the victim survivor’s self-esteem, confidence and capacity to resist controlling behaviour.
Common beliefs and attitudes
As described in Section 12, the common drivers of family violence in all communities are influenced by the gendered beliefs and attitudes of entitlement of the perpetrator in their personal, community and social context.
Perpetrators may express beliefs or attitudes about their own characteristics, circumstances and role in the family context. This includes gender-related social norms and extent to which they subscribe to heteronormative social norms.
They may also attribute beliefs and attitudes to, and expect them of, victim survivors. This includes expectations of gender norms and roles of an adult or child victim survivor. Perpetrators may express these beliefs as entitlement to authority, such as expectations the victim survivor will defer to them on family decisions.
They may expect women or older people to assume caring roles and look after family needs and children and support their (the perpetrator’s) life and career decisions without question.
They may also have expectations of behaviour of female or male children that perpetuate gendered norms and expectations.
In addition, they may have views about how family relationships should be conducted, rights to discipline and who has family decision-making rights, including across relationships between intimate partners, carers, adults and children and the extended family.
For example, a man may view themselves as physically and emotionally strong, invulnerable and virile. Within the family, he may view his role as the ‘owner’ of the family. This may be reinforced if he is the main income earner and view himself as the head of the household or family.
Finally, these beliefs may reflect ‘norms’ within a perpetrator’s peer group or community, which may reinforce or challenge a perpetrator’s use of violence towards family members. This includes widely held social norms such as gendered roles and adherence to heteronormative identity and ‘relationship norms’.
Structural and institutional factors
Similarly, perpetrators can use structural and institutional features of society to enact systems abuse.
They may use, leverage or manipulate systems to reinforce their coercion and control of victim survivors, or by engaging with services in ways that seek collusion.
For example, they may:
- make vexatious threats about parenting arrangements for children, threatening to report the non-violent carer to child protection or to disrupt immigration processes or visa status
- seek intervention orders against the real victim survivor
- access and use data or records from official sources as a method of continuing coercion and control, stalking and undermining of the victim survivor’s perceptions and experience of safety and wellbeing.
Perpetrators may also create barriers to community and institutional structures to further erode the victim survivor’s access to rights, services and other external support.
For example, they may undermine the victim survivor’s:
- ability to gain/maintain employment or education
- access to medical or support aids
- connection[69] to family, community and culture.
You should be attuned to the interplay of all these factors. They will vary in each situation and require you to understand the way in which power and control tactics manifest in different family and community contexts.
Presentations of family violence in different relationships and communities
How perpetrators use family violence behaviours across the community.
Understanding presentations of how perpetrators use family violence behaviours across the community starts with the recognition of the high prevalence experiences and the impact of family violence for:
- women and women as mothers (and carers) in an intimate partner relationship with the person using violence
- children and young people from the perpetrator (usually a father/parent or other carer).
This section is then structured to describe particular experiences of victim survivors in relationships with perpetrators within and outside of each community, including:
- victim survivors from Aboriginal community who experience family violence from both non-Aboriginal perpetrators and Aboriginal people who use violence
- victim survivors from diverse communities who experience family violence from people who may or may not identify with the same diverse community
- where victim survivors and/or the person using violence may each have specific complex health and mental health or compounding risk issues, of the same or other presentations.
Remember
Aboriginal people are recognised as our nation’s First Peoples. Aboriginal people are described throughout this document separately from ‘diverse’ communities.
Both Aboriginal people and people from diverse communities experience structural inequality, barriers and discrimination, and these are described in the following sections.
It is important to consider the victim survivor as a whole person when assessing how the perpetrator is targeting their family violence behaviours, as well as their access to your service.
For example, consider the experiences and barriers for people with disabilities and recognise this may be only one aspect of their identity.
The perpetrator may target the person’s other identities and experiences, which you also need to consider to ensure safe, accessible responses.
The information in the following sections will inform your understanding of how victim survivors from all communities can experience any combination of family violence risk factors, including and in addition to the specific common presentations of risk outlined in the victim survivor–focused Responsibility 7.
Note: Use of gendered language
The prevalence of family violence against women and children, and against women as mothers and carers, is well established and recognised across the service system.
Acknowledging this, when specifically talking about this predominant experience, this section uses gendered language, particularly in relation to:
- the predominant presentation of cisgender male perpetrators in intimate partner relationships with cisgender female victim survivors
- the experience of mothers, including damage to the mother–child bond caused by the perpetrator’s (predominantly the father’s) behaviours.
The term ‘mother/carer’ refers to any parent/carer who is not using violence (not a perpetrator).
Gendered language is not used when describing experiences of family violence towards and across LGBTIQ communities.
Further, there is a continually evolving evidence base suggesting similar rates and forms of family violence occur across LGBTIQ communities.[70]
Any shifts in use of gendered language are not intended to diminish any experiences of family violence, which can occur across all communities, gender identities and relationship types.
Men’s experience as victim survivors
Men can experience family violence. The prevalence of men experiencing family violence is a smaller proportion of all victim survivors, and is largely due to violence from other men.[71]
The experience of male victims is outlined in each section providing guidance on the experience and impact of risk across relationships, including against Aboriginal men, men from diverse communities and older men experiencing elder abuse.
Developing your knowledge
Continue to reflect on and develop your own knowledge about identities, barriers and experiences of family violence across the community.
If you lack confidence or feel ill-equipped to respond, you can engage in secondary consultation and referral with organisations that specialise in working with particular community groups (Refer to Table 2, and the victim survivor and perpetrator-focused Responsibilities 5 and 6).
12.1.1 Intimate partner family violence perpetrated against women
Family violence and sexual assault are the most common and pervasive forms of violence against women. Family violence is the greatest contributor to ill health and premature death in women under the age of 45 years.[72]
Key statistics[73]
- On average, one woman a week is murdered in Australia by her current or former partner.[74]
- Aboriginal women are 32 times more likely than other women to be hospitalised and 10 times more likely to die from violent assault.[75]
- Women and girls with disabilities are estimated to be twice as likely to experience violence as those without disabilities.[76]
Common perpetrator behaviours towards women
Common tactics perpetrators use towards women (usually by current or former male intimate partners) include:
- constant monitoring and regulation of her everyday activities such as phone calls, social interactions and dress
- evaluating her every move against an unpredictable, ever-changing and unknowable ‘rule book’[77]
- constant put downs about anything and everything she does
- having no control or say about the household finances
- criticism of her parenting skills
- disrespectful behaviour towards her in front of their children and others
- threats and actual physical violence against her, their children and pets
- being blamed for the violence
- surveillance using smartphones and other technology.[78]
Impacts of perpetrator behaviours
A perpetrator’s use of family violence can cause physical injuries, disability, miscarriage, sexually transmitted diseases and homicide of victims.
It can also result in indirect health or mental health-related symptoms for victim survivors, such as headaches, irritable bowel syndrome and self-harming behaviour.
As a result of a perpetrator’s use of family violence, victim survivors might also experience depression, fear, anxiety, low self-esteem, social isolation, financial debt, loss of freedom, and feelings of degradation and loss of dignity, and pre-existing disabilities and mental illnesses may be exacerbated.
Women who experience a perpetrator’s pattern of coercive and controlling behaviours over time are also likely to have trauma responses or to be diagnosed with posttraumatic stress disorder (PTSD). Symptoms include nightmares, flashbacks, emotional detachment, insomnia, avoidance of reminders (‘triggers’) and extreme distress when exposed to these, irritability, hypervigilance (watching for anger or signs of violence), memory loss, excessive startle response, clinical depression and anxiety, and loss of appetite.
Women with family violence experiences are up to six times more likely to use substances. This ‘self-medication’ can be understood as a way of coping with and managing the impact of trauma.
While every woman’s experience of family violence is unique, for many, the perpetrator’s abuse increases in frequency over time, rather than being a one-off incident.
Family violence often starts with an intimate partner’s apparent love transforming into family violence through use of controlling and intimidating behaviour. Over time, the perpetrator will increasingly isolate the woman from friends and family.
A perpetrator’s use of physical or sexual violence may not occur until the relationship is well established, or it may not occur at all. The perpetrator’s abusive, violent, threatening and controlling behaviours create an environment of fear and constant anxiety in their home and relationship where women and children should feel safe and secure.
Recognising common perpetrator presentations and narratives
Men’s use of violence against a female intimate partner is the most common and pervasive form of violence against women.[79]
Key statistics:
- Men perpetrate 90% of all violent crime in Australia.[80]
- Of the 2.2 million women who have experienced male intimate partner violence since the age of 15, 1.8million experienced physical violence and 0.9 million experienced sexual violence.[81]
- Nearly 1 million women had experienced multiple incidents of physical violence by the same man.[82]
- Women with a disability were more likely to experience multiple incidents of violence by a male perpetrator.[83]
Many men minimise their use of violence or abuse and seek ways to justify or avoid responsibility for their actions and their impacts.
In early conversations, men who use violence will describe the family violence as a ‘one-off incident’, related to being tired, stressed or pressured. This may shift over time to narratives that disclose patterns of violent and coercive behaviour.
This change may occur in response to managing or dismissing an internal narrative that they are inherently bad or problematic, which can relieve or minimise feelings of shame, guilt or taking responsibility for their behaviour.
Perpetrators rarely disclose physical or sexual violence in their interactions with the service or justice systems. It is more likely they will present a story about their life, relationship or family, or a specific and sometimes repetitive negative narrative about their current or former partner.
This can often take the form of criticisms and judgements of their partner, which may be subtle or overt.
Examples include:
- the lack of cleanliness or orderliness within the family home
- the use of finances, which the perpetrator may feel justified to direct due to their ‘breadwinner’ status
- complaining about or indicating non-support of their partner’s decisions or goals
- taking sides with those their partner might be in conflict with, for example, other family members
- always pointing out their partner’s shortcomings or failings
- complaining about their partner not understanding their position and the stresses they are under – from work, family life, finances or friends – nor supporting their coping mechanisms, such as excessive alcohol use.
During your engagement with men, you should develop a picture of the victim survivor’s identity.
In particular, take note of perceived ‘vulnerabilities’ the perpetrator may exploit to create isolation or control.
Some men, particularly those who have had multiple relationships where they have used violent and controlling behaviours, exhibit a pattern of choosing intimate relationships with partners they perceive to be ‘vulnerable’. In these situations, power dynamics are commonly exploited for control and domination, for example:
- non-Aboriginal men towards Aboriginal women
- Australian citizens towards non-visa holders
- able-bodied men to women with disability.
Service access and engagement barriers for perpetrators
The lack of help-seeking among men is a serious issue in the Victorian community.
Men’s help-seeking for emotional distress is consistently lower than that of women. This directly contributes to mental illness and maladaptive coping.
For example, men are almost three times as likely as women to have a substance abuse disorder[84] and are at greater risk of suicide.[85]
These issues can be linked to gender socialisation and gendered values associated with masculinity, such as stoicism and invulnerability.[86]
Research has explored the extent to which constructs of masculinity are either protective buffers or risk factors to men’s health. It finds that conformity to masculine norms are risks to men’s overall health outcomes, principally due to less help-seeking and negative attitudes towards psychological treatment.[87]
Although initial presentation to services is an important indicator, help-seeking should be understood as broader than the act of asking for help or seeking out a service.
Once a man has entered a service or begun a course of treatment, masculine norms related to self-sufficiency may interfere with treatment processes and lead to deficits in the therapeutic alliance.[88]
Fundamentally, service users engaging in services must believe that they cannot fix their problem alone. For men who hold ideals of invulnerability, the treatment process poses very particular challenges and threats to identity and self-concept.
Men who use or are at risk of using family violence are often able to identify a need for early intervention before their behaviour reaches the point of police and court-based intervention.[89]
However, this does not always translate to help-seeking, with a common barrier shown to be a lack of knowledge about the specific points, places, and contexts in which opportunities to engage with help might exist.
A proportion of men are willing to access professional help, but the ways that such help is presented to them is of particular importance.
12.1.2 Family violence against parents/carers (usually mothers/women) [90]
Perpetrators’ use of family violence impacts on non-violent parents who are usually women, other caregivers, kin or guardians.[91] [92]
Perpetrators often use various harmful tactics to deliberately undermine, manipulate and damage the mother/carer–child relationship.
This may be based on social norms and gender stereotypes about women as primary carers who are responsible for children’s health, wellbeing and development.
This will be affected further if the perpetrator has control over financial resources required for parenting.
Professionals need to be aware of these tactics to avoid making judgements about women’s parenting.
The way a woman may resist the violence can be misinterpreted by professionals and others as ‘poor parenting’.
Tactics perpetrators use to damage the mother–child relationship can include:
- threatening to use the family law and child protection system to attack and undermine the mother–child bond
- creating an environment of instability and harsh discipline in the home
- conditioning children to misinterpret their use of coercive and controlling tactics and its impact on the family in a way that leads children to blame their mother, minimise the abuse and distance themselves from her (this is sometimes called ‘maternal alienation’)
- actively belittling women in front of their children through emotional abuse, name-calling, intimidation and humiliation (such as expressing sexual jealousy)
- isolating women from their friends and family and preventing them from accessing services to support their parenting.
Impacts of perpetrator behaviours
These perpetrator tactics have significant emotional, social, health and financial impacts on women and their mothering, causing women to lose confidence in their parenting; and affecting their ability to be as engaged with their children as they want to be.
The experience of family violence is exhausting, distressing and isolating. As a result, women may be less attuned to their children’s needs.
The perpetrator’s tactics of coercion and control may affect a woman’s ability to parent in a number of ways.
Several studies have found that perpetrators’ use of family violence results in women having a reduced sense of control over their parenting.
This is often made worse because of a perpetrator’s control of financial and material resources, leaving women with few resources to look after their children, such as paying for nutritious food or school excursions.
In this environment, the woman may find it difficult to be an available, energetic, patient parent, to focus attention on her children’s needs, and to keep track of all the various tasks that parenting requires.
Also, if a woman’s parenting is being heavily criticised by her partner, she may lose confidence and develop an indecisive parenting style.
She may also overcompensate for the perpetrator’s abusive or controlling behaviour towards children by not creating or maintaining healthy boundaries for them.
The constant stress and pressure experienced by women who are struggling to care for and protect their children while being targets of violence may manifest as depression, anxiety or substance abuse. This can further affect their parenting and relationships with their children.
Children experiencing family violence may also display behavioural issues and have complex emotional needs that present further parenting challenges. Sometimes this results in further criticism of her parenting by the perpetrator, professionals or others.
Identifying and responding to situations where these behaviours present as adolescent family violence is described in the victim survivor–focused MARAM Practice Guides.
Practice considerations
Practice considerations for responding to parent/carers experiencing family violence include, but are not limited to the following:
Increased risk of harm
- The perpetrator’s violence often escalates when the woman/partner is planning to leave or has left the relationship, with an increased risk of assault, stalking and murder for both women and their children.
- Many family violence homicides occur during the separation period.
Decreased availability to children
- The perpetrator is jealous of her time/attention given to her children.
- The perpetrator interrupts breast-feeding, meal-time, story-time, sleeping routines.
- The perpetrator actively draws her attention to him when her attention is being given to the children.
- The perpetrator expects her to do all the care of children and household tasks without assistance from him.
Financial pressures
- The perpetrator withholds money and other resources.
- Loans and other debts or credit contracts may be taken out in her name.
- She may have to leave her job if she needs to be relocated for safety.
- This affects children because of the lack of material resources to support them.
Conflicting concerns and priorities
- Not wanting to disrupt her children’s lives, education, and links to family and community.
- Believing it is in her children’s best interests to be close to their father.
- Believing she is protecting her children from the violence by ‘hiding’ it from them.
- Continuing to care for her partner and hoping he will change (many women do not want to leave the relationship – they just want the violence to stop).
- For some Aboriginal women, the fear of risking their connections to extended kinship and family networks and to land or country.
- For some women with disabilities, reliance on, or the fear of losing a family member from whom they receive disability support.
- For some immigrant and refugee women, the fear of losing their visa status or residency entitlements.
- Wanting to avoid the stigma associated with being a single parent.
Social isolation and its effects
- The perpetrator prevents her from leaving the house, engaging socially or with family, or accessing support to parent.
- Feelings of shame and guilt about the violence and its impacts on her children, or believing it is her fault.
- Fear of being isolated or ostracised by her community or culture.
- Fear of being judged by others, particularly about her parenting.
- Difficulty making decisions because she has been cut off from friends and family, is exhausted, and/or lacks confidence in her own judgement.
Barriers to accessing the system
- The perpetrator attends all appointments with her or does not allow her to access services.
- Women experiencing family violence may not know there are support services that can help them.
- Women may not know about the kinds of support available to them; they may feel that services will not be able to help with their situation.
- Women may be concerned that services or professionals will judge their parenting negatively.
- Women may not have access to money and may not know where financial support is available.
- A lack of safe, accessible and affordable housing means women may have limited options or may not be aware of their available options.
Recognising common perpetrator presentations and narratives
Family violence often commences or increases in frequency and severity during pregnancy. At this time, perpetrators can feel that their position or role in their partner’s life is threatened and that their partner is emotionally detaching from them.
They may also feel fearful of decreased connection and/or intimacy and create unhelpful thoughts about rejection.
Lack of intimacy and emotional connection, including during sex, can feel threatening to some men and the loss of this can leave them feeling abandoned. Increased controlling behaviours can commence or escalate quickly at this time.
Some men will openly disclose deep resentment about their partner, stemming from the time of pregnancy. They may express this with statements like: ‘she’s been cold’, or ‘everything changed when she got pregnant’.
Following the birth of a child, men may disclose feeling that they are not ‘needed’ or are ‘superfluous’ to the emotional sphere in the family home.
They may feel that their ‘expectations’ or feeling of entitlement to sexual connection and intimacy are no longer being met by their partner.
Perpetrators often take the role of parental expert, pointing out the other caregiver’s shortcomings. They may present these narratives through criticism, including:
- how the mother or other caregiver is failing the children and them in their parenting
- blaming the mother/caregiver’s parents for their partner’s parenting approaches and learned skills
- dismissing the other caregiver’s parenting and ridiculing them in front of the children or others
- presenting as the expert in a very logical way in public that further humiliates the other caregiver, including making complaints to schools and child protection
- focusing on children’s medications and health issues and the perceived inability of the mother or other caregiver to manage the issue
- removing or reducing the mother’s ability to breastfeed by destroying stored breast milk or forced weaning
- disappointment or anger at the lack of physical intimacy since having children or increased pressure for sexual intercourse
- blaming adolescent children’s challenging behaviours on the mother/other caregiver, claiming they are responsible for ‘not bringing the children up in the right way’ and being ‘too soft on them’, and that this is the reason for current behaviour.
Service access and engagement barriers for perpetrators
People using family violence can often feel resentful towards their partner or other caregiver if pushed to engage with services.
These narratives serve to block the process of responsibility-taking, inviting collusion from professionals.
Men’s Behaviour Change Program participants have been found to hold varied attitudes towards their current or former partner, ranging from wanting to restore their relationships to verbalising significant anger and resentment.[93]
People using family violence have varied levels of motivation to take steps towards safety and change for the benefit of their partner or other caregiver. For professionals who have a role to work with parents who use violence, the focus of intervention is creating a safe and appropriate co-parenting relationship, for the promotion of children’s safety and wellbeing.
Acknowledging pregnancy and new father/parenthood is a useful opportunity for the person using violence to discuss how they are feeling, thinking or responding to their new situation, and for professionals to hear the narrative they are constructing about their partner and about themselves in this new role.
12.1.3 Family violence against children and young people
Children are victim survivors of family violence in their own right, whether they are directly targeted by a perpetrator, or they are exposed to or witness violence or its impacts on parent/carer and/or other family members.
Exposure to family violence is a significant risk factor that impedes the development, safety and wellbeing (including education) of children and young people.
Children and young people do not have to be physically present during violence to be negatively affected by it, or to be considered victim survivors.
Exposure to violence can include:
- hearing violence
- being aware of violence or its impacts
- being used or blamed as a trigger for family violence
- seeing or experiencing the consequences of family violence, including impacts on availability of the primary caregiver and on the parent–child relationship.
Essentially, where a child is part of a family in which a perpetrator is using family violence, they must be considered a victim survivor of that violence in their own right, even if they are physically removed from the situation (such as staying with friends or another family member).
It is important to note that children have historically not been understood as victim survivors in their own right, and their specific wellbeing and safety needs have not been adequately identified or addressed.
For example, a disciplinary approach may be taken by professionals to children or young people displaying challenging behaviours, without considering that this behaviour may be the result of exposure to family violence or other abuse.
Infants are especially vulnerable due to their reliance on adult caregivers, yet they are least likely to receive a service response.
This has reduced the evidence and data available, and it means outcomes for children are not well understood and therefore only limited specific practice responses have been developed.
Siblings are likely to be affected differently by the experience of family violence, and it is important to understand the different developmental impacts of family violence across the life span.
For example, a toddler may not be able to speak about their experience of family violence but may display cognitive or behavioural changes or issues.
Younger children are also likely to have different risks and needs to an older child or young person, given their stage of cognitive, social and emotional development.
Guidance on observable signs of trauma that may indicate family violence are outlined further in victim survivor–focused Responsibility 2.
In the MARAM Framework, ‘unborn children’ refers to those in-utero during pregnancy, ‘children’ are considered to be those under the age of 18, and ‘young people’ specifically refers to older children, typically adolescents and pre-adolescents 10 years of age and older.
Because children and young people are dependent on adults, and as they are still developing physically, cognitively, emotionally and socially, they are especially vulnerable to the long-term impacts of family violence.
While this section specifically refers to people younger than the age of 18, the characteristics, impacts and barriers discussed in this section may apply to other age groups.
For example, the term ‘young person’ is commonly used to refer to people aged up to 21, or sometimes 25, noting that many young people older than 18 years of age remain in the care of their parents and are not living independently, and that brain development continues at least up until age 25.
There is now a strong evidence base that shows:
- the effects of physical and emotional violence and abuse experienced by women during pregnancy can affect the unborn child and their brain development at a very early stage
- negative experiences in the first three years of life have long-lasting effects on brain development, especially where a child’s primary attachments (that is, their relationships with their primary caregivers, usually parents) are undermined or compromised
- because early childhood attachment, safety and wellbeing provide the foundation for physical, social and emotional development, learning, behaviour and health through school years and into adult life, trauma during this period can have significant lifelong effects. For example, later in life, they are more likely to abuse substances, be involved in crime, lack skills in maintaining respectful relationships with others including partners, and have poor parenting practices
- multiple negative and traumatic experiences can have a compounding effect where the impact of each trauma is multiplied, which is sometimes referred to as ‘cumulative harm’
- young people who experience family violence (or other forms of abuse) have a higher risk of either experiencing further violence in their future relationships, or perpetrating violence themselves.
Impacts of perpetrator behaviour and use of family violence on children’s familial relationships
The attachment of children and young people to parents and caregivers is key to their development, safety and wellbeing, and can be significantly impaired by family violence.
The relationship between a caregiver, who is a victim survivor, and their child is often affected by the perpetrator’s pattern of coercive and controlling behaviour.
For example:
- children might feel unable to trust that their mother will protect them, particularly as perpetrators often undermine her parenting or manipulate the children’s perception of their mother. This may be compounded if the impact of the violence on children has not yet been acknowledged
- women may believe they are protecting their children from violence by ‘hiding’ it from them. Conversely, older children and young people may also try to hide these impacts from their mother, seeking to protect her from further distress
- professionals may interpret children’s behaviour as ‘difficult’ or ‘defiant’ without realising that children and young people are experiencing significant psychological, emotional and behavioural consequences of family violence, including anger, fear, trauma, sadness, shame, guilt, confusion, helplessness and despair. Additionally, older children and young people may withhold information from professionals because of a sense of shame or guilt
- children and young people may also feel a sense of loyalty towards the perpetrator, especially when the perpetrator is their father, which can create significant stress and tension for them. Sometimes perpetrators can appear caring and loving to their children, while manipulating the children’s attitudes towards their mother, or may be alternately loving and abusive to the children.
As children and young people’s emotional maturity is still developing, they may be less equipped to understand and cope with the complexity of a situation where one parent is using violence against another (or against the child themselves). This poor modelling can affect their understanding of healthy and unhealthy relationships.
This can contribute to an intergenerational cycle of violence, with children and young people who have experienced abuse or violence at higher risk of experiencing victimisation (women) and perpetration (men) in their own intimate relationships.[94]
Trauma-informed approaches to children experiencing family violence
Where young people have experienced family violence, abuse and/or neglect, it is important to use a trauma-informed approach that is appropriate to their age and developmental stage.
This means considering how past experiences may affect their behaviour and wellbeing, and what kind of support is required to assist them effectively. Indicators of trauma for children and young people are outlined in victim survivor–focused MARAM Practice Guide for Responsibility 2.
Young people who use violence in the home or with an intimate partner must be provided with responses that prioritise the safety of victim survivors and ensure the young person takes responsibility for their harmful behaviours, while providing developmentally appropriate wellbeing supports to that young person.
Young people using violence may also be victim survivors at the same time.
Family violence is a key cause of stress in children and young people and can significantly disrupt healthy brain and personality development.
Recent evidence indicates that ongoing exposure to traumatic events as a child, such as witnessing or being the victim of family violence, results in chronic overactivity of the body’s stress response and changes to the brain’s architecture.
This can lead to behaviours such as hypervigilance and hyperactivity, affecting them throughout their lives. In serious cases, this can lead to deficits in learning, behaviour and physical and mental health and wellbeing.
Service access and engagement barriers for victim survivors
- Children and young people are often not considered to be victim survivors in their own right, instead being considered primarily or solely through their relationship to an adult victim survivor, leading to inappropriate or inadequate responses.
- Children and young people are often not directly engaged by services, due to professionals lacking confidence, or holding a view that children’s safety and wellbeing is not directly their responsibility (for example, the responsibility of the parents, or another service such as child protection).
- Responses to children and young people who use violence in the home may not be developed to respond to their specific and potentially ongoing therapeutic needs.
- Children and young people may continue to experience significant impacts of family violence after the violence has ended, because they often must continue to navigate a relationship with the perpetrating parent in shared custody arrangements.
- Often the parents’ desire for contact with their children — or the child’s expressed wishes to see their father, for example — are prioritised by families and courts over the safety of the child, even where there are intervention orders in place. This decision may assume that continued contact with their father is beneficial for the child .[95]
- Those under the age of 18 years face particular difficulties in accessing services in their own right and are more or less reliant upon an adult parent or guardian’s decision-making.
- Children and young people may legally have their will and preference overruled by adult consent, even where their response to the family violence differs.
- Children and young people have limited means to deal with their exposure to violence or express that they are experiencing violence. This may be compounded if they do not understand perpetrator behaviours as being ‘family violence’, especially if this behaviour has been normalised for them.
- Perpetrators may actively prevent children or young people from accessing services (or prevent their mother from taking them) or threaten or coerce them into not disclosing to professionals.
Practice considerations
When responding to children and young people experiencing family violence, practice considerations include but are not limited to the following:
- Children and young people must be considered victim survivors in their own right, with their own experiences of family violence. This includes having specific threats, risks, protective factors and risk management approaches. All interventions must be considered for their impacts on every victim survivor, including children and young people.
- Responses to children and young people should take into account their age and developmental stage, as risk is likely to present quite differently depending on the age and maturity of the child.
- Where it is safe, appropriate and reasonable, a child or young person should be directly engaged with to ascertain their assessment of their risk, their identification of risk factors and their consideration of risk management strategies.
- Where it is not safe, appropriate and reasonable to engage directly with a child or young person, services should seek to collaborate with the parent who is not using violence or other professionals who interact with that child (such as schools) to ensure accurate and detailed information about the child or young person’s experience is collected and assessed.
- The child or young person’s relationships with other family members must be a core consideration of their risk assessment and management plan. This should include prioritising their safety in the context of any relationship with the perpetrator and promoting and supporting positive relationships with other family members, particularly the parent who is a victim survivor.
The wellbeing and safety needs of all children should be considered a core element of any response to family violence, and services should collaborate as appropriate to address these needs.
Recognising common perpetrator presentations and narratives
Men/parents who use family violence often have significant, ongoing parenting roles with children in their care.[96]
In your engagement with parents who use violence, it is important to identify whether there are children in their care, and the nature of the relationship, including contact and parenting arrangements.
While some parents/fathers disengage completely from the family following family violence and separation, there is higher risk associated with those who continue to have relationships with their children, or a strong desire to, despite parenting or intervention orders preventing or limiting this.
This is due to the proximity and opportunity to continue to use violence against children in their care, and/or use the parenting role as a continuation of violence against an adult victim survivor/parent.
When working with fathers/parents who use violence, you should focus the intervention on the expectation of high parenting standards to increase children’s safety and wellbeing.
When working with parents/fathers, you may hear or observe attitudes and narratives that indicate potential risks of them perpetrating family violence, including:
- a sense of entitlement or self-centred attitudes relating to children/parenting role
- overcontrolling or harmful parenting behaviours
- overuse of physical forms of discipline (hitting, smacking)
- anger demonstrated towards their children
- holding unrealistic expectations and poor understanding of child development
- denying any problems in their relationships with their children
- considering themselves to be good fathers
- acknowledging ‘mistakes’ in their parenting, often explaining this as a one-off (or minimising, justifying or blame-shifting to the other parent/carer)
- believing that their use of family violence had little impact on their children
- strong gender roles and expectations that differ between male and female children
- negative beliefs or attitudes in the value of non-biological, particularly male, children.
Some men also present as trying to ‘rescue’ their female partners from her single-parenting duties or previously violent relationships.
This may indicate a level of precursor controlling behaviour from entitlement and role as ‘protector’.
For example, a perpetrator may threaten a partner’s capacity or ‘right’ to children.
This may take the form of attacking the mother/parent–child bond, undermining their ability to parent, and by exacerbating fears linked to negative experiences of government service interventions.
This is particularly acute among Aboriginal communities who have experienced current and historic discriminatory government policies removing children from their families and communities.
In working with fathers/parents who use violence, it is important to understand the different behaviours or parenting approaches that are directed towards each child within the family unit.
At times, there will be particularly stark differences between the type of violence or control directed at:
- biological children versus stepchildren or other children in their care
- male compared with female children
- children with identities that are different to one or both parents.[97]
Service access and engagement barriers for perpetrators
The perpetrator’s role as a parent can be a significant motivator for behavioural change.[98]
The Royal Commission noted that ‘for men new parenthood is a time that they may be more open to receiving information and skills development, as well as to considering alternative models of masculinity as they move into a new parental role’.[99]
Engaging and intervening with people who use family violence who are birth parents or have an ongoing parenting role is an important component of promoting children’s safety, wellbeing and development and supporting the non-violent parent to keep children safe.
However, interventions designed for working with parents/fathers may at times be misused by the perpetrator.
This may present as an opportunity to continue using controlling and abusive behaviour, in particular when they attempt to use attendance at a program as ‘proof of their competence as a father/parent’.[100]
Despite this challenge, when services do not proactively engage parents/carers who are using violence, a greater burden and unwarranted focus is placed on non-violent parents/carers and children who are engaging with the service.
This can result in non-violent parents/carers, often mothers, being blamed for ‘failing to protect’ their children and provided inappropriate interventions, rather than holding the parent/carer using violence responsible for exposing children to harm or directly using violence against their children.
If parenting is identified as a potential motivator, you should consider if it is safe, appropriate and reasonable in the circumstances to use this motivator, given the risk level for adult and child victim survivors, and the wellbeing and needs of the child or young person.
You should also be aware if there are system interventions, such as court-ordered parenting arrangements in place or intervention orders preventing contact.
Refer to the perpetrator-focused Responsibilities 3, 4, 7 and 8 for further guidance on using parenting as a motivator for engagement and change.
12.1.4 Family violence against Aboriginal people and communities
Aboriginal definitions of the nature and forms of family violence are broader than those used in the mainstream and reflect that Aboriginal families include extended family, kin and other community members who may not be directly related.
Family violence contributes to overall levels of violence reported by Aboriginal people and the trauma experienced within families and across family and community networks.
The use of family violence is not part of Aboriginal culture. The assumption that family violence is part of Aboriginal culture is an oppressive statement that creates barriers to people accessing services and taking accountability for changing behaviour.
This can also be internalised by young Aboriginal men, who may have grown up experiencing or witnessing family violence.
Since colonisation, Aboriginal people have experienced high levels of family violence, largely perpetrated by non-Aboriginal people against Aboriginal women and children at significantly higher levels than that experienced by non-Aboriginal women.[101]
Aboriginal women are 32 times more likely than other women to be hospitalised and 10 times more likely to die from violent assault.[102] Aboriginal men can also experience family violence.
Higher prevalence of family violence against Aboriginal people, particularly Aboriginal women, is due to a number of factors, many of which relate to the generational impact of colonisation, invasion and dispossession on Aboriginal culture and communities.
Aboriginal people experience multiple and intersecting forms of inequality and discrimination relating to culture, gender identity, sexuality, ability, spirituality and age which can compound barriers to accessing services and increase disengagement with formal supports.
Service access and engagement barriers for victim survivors
There are many barriers to seeking help for Aboriginal people experiencing family violence.
These can include past and recent experiences of systemic, individual and collective racism, judgement, unconscious bias or privilege or a lack of cultural competency from services.
Systemic discrimination in the form of current and historical policies continue to affect Aboriginal people, families and communities. This creates mistrust and uncertainty in what to expect from services and their cultural relevance.
When working with Aboriginal people, families and communities, it is also important to recognise the impact of current and historical forcible child-removal policies, including family separation and disconnection from culture and country.
This presents a barrier for Aboriginal people to engage with or trust mainstream community services, as well as statutory services and justice agencies. It is important to also recognise the ongoing impact of institutionalised abuse and neglect suffered by many removed children that continues to affect Aboriginal people, families and communities.
This is reinforced with experiences of discrimination, oppression and racism within and across the community from the predominantly white dominant culture/community.
You will need to consider what this means in the context of risk and impact to the person experiencing family violence, or the person using violence.
You should also proactively remove barriers by considering and applying the principles outlined in this guide and victim survivor and perpetrator-focused Responsibility 1.
Practice considerations
Practice considerations for responding to family violence used against Aboriginal people include the following:
- Use a strengths-based, self-determination approach that values the strengths of Aboriginal people and the collective strengths of Aboriginal knowledge, systems and expertise — and refer to and apply the Dhelk Dja principles for addressing family violence.
- Be aware that the person using family violence or the person experiencing family violence may not be Aboriginal. The majority of family violence against Aboriginal adults and children is perpetrated by non-Aboriginal family members.
- Family violence against Aboriginal people can include perpetrators denying or disconnecting victim survivors from cultural identity and connection to family, community and culture, including denial of Traditional Owner rights. This might include people using violence exploiting lack of connection to or contact with families, culture and supports for members of the Stolen Generations who have lost contact with families of origin. Isolation from community and culture are significant concerns and are highly impactful for Aboriginal people.
- Aboriginal people may be reluctant to seek help that involves leaving their families and communities, given previous policies of dispossession and removal, including the Stolen Generations, and current high rates of child removal.
- Aboriginal children are overrepresented in child protection matters, particularly in the context of family violence. Professionals should support parents/carers seeking assistance and acknowledge and respond to fears about child protection and the possibility of children being removed from their care.
- Aboriginal people may be concerned that seeking help will create conflict in the community. For example, given the high rates of Aboriginal deaths in custody, some community members may negatively view a victim survivor’s engagement with the police and justice system. When assessing risk to Aboriginal people, you should keep in mind the context of violence and potential repercussions from other Aboriginal family members if action is taken.
- Professionals should support both Aboriginal adults’ and children’s cultural safety when undertaking family violence risk assessment and management. This means recognising inherent rights to family, community, cultural practices and identity, including when working with Aboriginal children with non-Aboriginal parents and family members. Responsibility 1 provides further guidance on cultural safety.
- Many Aboriginal people may prefer to use Aboriginal services. It is important to provide choice and service options for Aboriginal people experiencing family violence. If a family member is Aboriginal, whether they are a victim survivor or another family member, professionals can offer to connect with Aboriginal community-controlled organisations for family violence support (also refer to victim survivor–focused Responsibilities 4 and 5).
Recognising common presentations and narratives of people using violence
If the person using violence is non-Aboriginal, read this section in conjunction with the previous sections on the gendered drivers of family violence.
White men and men from dominant cultures and positions of power or privilege may seek to collude with professionals to exploit systemic discrimination and bias of systems and professionals against Aboriginal victim survivors.
All people using violence use common narratives including denial, minimisation, blaming the victim survivor for their use of violence, claiming to be the ‘real’ victim and justifying their use of violence.
These narratives may focus on the person’s own experience of family violence or trauma, to minimise or reduce responsibility for their violence against adult and child victim survivors.
Non-Aboriginal people using violence towards Aboriginal family members may present with narratives that attempt to use systems abuse by seeking collusion from services.
They may do this by presenting as charming or attempting to draw parallels between their own (often) white, dominant-culture male privilege and capacity and that of the professional or service. Their aim may be to exacerbate discrimination, avoid responsibility and undermine victim survivors’ access to services.
They may use negative language or make inaccurate reports to police or child protection, to misidentify an Aboriginal victim survivor as using violence as a tactic of coercive control.
People using violence towards Aboriginal victim survivors may seek to prevent them from accessing their family, community or culture for support.
They may use derogatory language about the victim survivor’s Aboriginal identity as a tactic to belittle and isolate the Aboriginal victim survivor.
The person using violence may use coercive control to force an Aboriginal victim survivor into illegal activities, exacerbating and compounding ramifications for Aboriginal victim survivors who are overrepresented in justice systems.
Violence may also be occurring beyond intimate partner relationships, within the broader family or community.
Professionals must consider these extended family relationships and unique dynamics, to identify any other coercive and controlling behaviour.
Stereotypes of Aboriginal women’s use of violence
Some services and professionals may hold biases about Aboriginal women being violent.
In this context, it is important to consider the realities of violent resistance.
Women may use force in response to patterns of violence from a predominant aggressor or person using violence. This results in many women being misidentified as a perpetrator.
Supporting women who use force requires a different risk management approach than responding to predominant aggressors/people who use family violence, due to intersecting structural inequalities, including those based on gender.
This approach must prioritise their risk management as victim survivors of family violence, and it can be supplemented with information on safety planning for self and their families.
Services must be aware that non-Aboriginal men using family violence may be more likely to exploit service stereotypes about Aboriginal women being violent.
By employing this stereotype, they can position themselves as the ‘victim’ (adopt a victim stance) and invite systems to collude with this narrative, leading to a misidentification of the (real) victim survivor.
Non-Aboriginal men who use family violence often use their position of privilege and confidence in using the service system to seek collusion from services and professionals to represent their own position or to further perpetrate systems abuse.
This may exacerbate barriers for Aboriginal victim survivors in receiving services, such as through increased fear of child removal for adult victim survivor parent/carers.
Service access and engagement barriers for perpetrators and people using violence
If working with a non-Aboriginal man using violence against an intimate partner, refer to guidance about service access and engagement barriers in previous sections. These include help-seeking and attitudes and feelings towards victim survivors including parenting responsibilities.
In addition to these barriers to engagement, non-Aboriginal people who use violence towards Aboriginal family and community may present with specific tactics that invite collusion from professionals and exploit their privilege to ‘make invisible’ their own violence.
Where services and professionals recognise these tactics and behaviours, it is important to respond using a balanced approach to keep the person engaged with the service system (refer to Responsibility 3). Identify opportunities to work collaboratively with other professionals to minimise further systems abuse and exploitation.
Aboriginal people who use violence also experience similar service access barriers that Aboriginal victim survivors experience. This is due to systemic inequality, barriers and discriminatory policies, practices and systems.
Aboriginal people using violence also live within the context of historical and current dynamics in which family violence occurs. This includes the impacts of colonisation, loss of culture, trauma accumulated across generations, access to employment, connection to Country and kinship relations, and the historical and current impacts of forced child removal.
Services and professionals must avoid stereotypes and biases related to family violence in Aboriginal communities to prevent additional barriers for Aboriginal people to access services.
Aboriginal-led programs have an essential role to play in modelling healthy, respectful relationships to support Aboriginal men to reconnect to culture and Country, and to maintain and preserve safe and respectful behaviours in their relationships.
Practice considerations for responding to Aboriginal victim survivors will also assist you to engage with an Aboriginal person using violence. Some additional things to consider include the following:
- Apply Dhelk Dja principles, culturally safe, trauma and violence–informed practices, led by a self-determination approach and empowering individuals and community in all engagement to actively address service access barriers.
- Focus on safety for self and safety for family and community, being aware of and supporting the need for Aboriginal-led holistic healing and therapeutic services for people who use violence, while holding and promoting accountability from the beginning of engagement.[103]
- Use a person-centred, ‘person in their context’ approach, to consider the meaning and significance of connections to family, community and culture for the person using family violence. Seek cultural consultation to provide a culturally safe trauma-informed approach.
- Reflect on the potential consequences of your engagement and actions to the safety and wellbeing of adult and child victim survivors and community.
- Understand that Aboriginal people may choose to use mainstream services at times, for example to maintain anonymity, and all services must be prepared to provide a culturally responsive and safe response.
12.1.5 Family violence against older people (elder abuse)
Elder abuse is a form of family violence. In the Victorian family violence context, this is defined as any behaviour of a perpetrator as defined in the FVPA where it has occurred within any family or family-like (including unpaid carer) relationship where there is an implication of trust, and which results in harm to an older person.[104] This includes any family violence risk factor that applies to an adult victim survivor from a perpetrator’s behaviour.
There is growing recognition of elder abuse as a form of family violence, and greater attention on how the family violence service system responds to older people. This is enhancing the evidence base of prevalence and best-practice responses.
It is important to recognise that older people are a diverse cohort. All older people can experience family violence.
Most older people live independently and do not require care or support; however, they can still experience violence from adult children and other family members.
Given the prevalence and impact of family violence from adult children, this guidance has a particular focus on older people who do require care and support – as well as where an adult child is themselves in a period of transition and is relying on an older person for care and support.
As with all family violence, some forms of abuse may constitute criminal acts, such as financial[105] , physical, sexual abuse and neglect.[106]
An adult child who misappropriates their parent's finances may have committed a crime such as theft if they have not sought permission to take the funds and have no intention of returning them.
Elder abuse may be the continued experience of family violence from intimate partners which may have occurred over a number of years. It may have commenced or escalated more recently. For older people experiencing intimate partner violence, the perpetrator profile is generally the same as if they were a younger person experiencing intimate partner violence.
The use of power and control by a perpetrator of elder abuse is similar to that used by perpetrators of intimate partner violence. However, some forms of elder abuse can have a different perpetrator profile.
Older people can also experience forms of elder abuse from other family members, such as intergenerational abuse (for example, from an adult child to parent/s or grandchild/ren to grandparent/s).
Women remain over-represented as victim survivors of elder abuse generally, however, more men experience abuse as an older person than in other contexts. The perpetrator profile can also differ, where for example, women are more likely to be perpetrators in situations of intergenerational abuse than in other contexts.
In addition to gender, the drivers of elder abuse can also include ageism. When not perpetrated by an intimate partner or carer of the person experiencing family violence, elder abuse is most commonly recognised as perpetrated by adult children.
It commonly manifests as financial abuse from adult children or other family members arising from ageist attitudes of entitlement to a parent or relative’s assets.[107]
Older people are recognised as an at-risk age group as they may be in a period of transition, which can increase dependence on family/carers.
This transition may create real and/or perceived ‘vulnerabilities’ that are targeted by perpetrators of elder abuse. This may also lead to discrimination from services or by society at large due to broader ageist attitudes.
Perceived vulnerabilities can include:
- recent loss of a spouse
- declining or diminished mental capacity or physical health from age-related diseases
- becoming marginalised and devalued due to ageism
- social and community connections diminishing over time, leading to isolation which increases susceptibility to mistreatment and abuse
- loss of economic power, or the accumulation of substantial assets
- language or financial literacy barriers reducing access to information, services and resources
- dependence on others
- poor or limited housing options.
Dependence is not a defining characteristic of family violence. In some situations, the older person may be independent but is supporting the person using family violence, particularly in providing housing or financial support.
For example, adult children with a history of perpetration or who are currently using family violence towards their partner or another family member, may return home and perpetrate violence against their parents.
Adult children may be receiving support from their parents in relation to use of alcohol and drugs, gambling and/or criminal activity.
Older people may feel obligated to support their children in these situations.
Service access and engagement barriers for victim survivors
Older people sometimes want to protect their family relationships and will put the needs of other family members before their own.
They may be more likely to seek alternatives to legal pathways when reaching out for assistance, as they simply want the perpetrator’s behaviour to stop.
Older people may try to avoid any further justice or legal consequences for the perpetrator in the hope of preserving the relationship, reducing further abuse or not wanting the perpetrator to ‘get into trouble’ from police and justice interventions.
How older people are considered within family and community relationships can be deeply bound to culture or faith.
Violence against older people must be informed by a recognition and understanding of their family structure, cultural or faith background.
There may also be gendered and normative expectations of women to remain in abusive relationships, or that family violence matters should be dealt with privately or within the family.
Some older people may believe abusive behaviour is a normal part of relationships or of ageing or hold fears that if an abusive caregiver is removed, they will lose access to care, or will face an unchosen change in living circumstances.
Violence against older Aboriginal people must be informed by an understanding of the context of Aboriginal family violence. This includes their many-layered experiences, the importance of familial and community roles that Aboriginal people and Elders hold, and the relationships of Aboriginal families and communities. You can work collaboratively with other services with expertise in this area to improve your understanding and response, if needed.
Other family members may also notice controlling or abusive behaviours but may feel unclear about who to turn to for support. They may also not want to exacerbate family tensions or other relationship issues.
This may signify unconscious biases and ageism, leading to a perception that elder abuse warrants less attention or need for intervention than equivalent forms of family violence occurring in other relationships and community contexts. This can be particularly true for intimate partner violence between older people. Family members or services may have an assumption that:
- intimate partner violence does not exist in older relationships
- violence from an older intimate partner is less severe than that perpetrated by younger intimate partners
- that ageing limits a person’s sexual expression or the likelihood of sexual abuse.[108]
These incorrect assumptions can be blind spots that affect the way services provide access, and assess and respond to risk, as professionals may not recognise behaviour as controlling or abusive.
Seek secondary consultation with specialist services to provide safe responses to older people, including Aboriginal Elders or older people from diverse communities, and refer to victim survivor–focused Responsibilities 5 and 6.
Specific practice considerations relating to all MARAM Framework risk factors for older people are outlined in victim survivor–focused Responsibility 7.
Practice considerations
Practice considerations for responding to older people experiencing family violence (elder abuse) include, but are not limited, to the following:
- Be aware of ageism from services and your own potential for unconscious bias and ageism. This can include not recognising their experience as family violence or undermining the person’s agency, such as by not engaging with them directly but instead engaging and potentially colluding with adult children who might be perpetrators.
- Be careful not to assume someone is incompetent or has cognitive disability (including dementia) based on how they present or communicate, particularly as they may be experiencing trauma or grief or depression. Capacity and competence should always be presumed unless the engagement, information gathering and secondary consultation suggests this is affected. Key principles and obligations under the Medical Treatment Planning and Decisions Act 2016 (Vic) and Guardianship and Administration Act 2019 (Vic) should guide response to older people with a disability or whose cognitive capacity is affected. These include:
- A person should be presumed to have capacity unless there is evidence to suggest otherwise.
- Capacity can fluctuate — a person may have decision-making capacity for some decisions and not others, and this may be temporary or permanent.
- A person has decision-making capacity if appropriate supports and adjustments can overcome any capacity issues.
- Professionals should not make assumptions based on the person’s appearance or the perceived merits of decisions they make.[109]
- For older people with cognitive disability, capability to engage with services, including self-assessed levels of risk may be affected. Ensure appropriate supports and adjustments are provided for older people with disabilities or whose cognition is affected to address any issues with capacity.[110] This may include communication supports (for example, speech pathologists), formal or informal advocacy, and different communication strategies (written, Easy English, and verbal reiteration).
- Be careful not to assume someone is incompetent or has dementia based on how they present when they may be experiencing trauma, such as how this is expressed as grief.
- There are few specialist services working with older people experiencing family violence. Universal services might not be aware of relevant services and how to connect service users to them. Professionals can connect and collaborate with different services in relation to issues arising from family violence, such as financial and legal services to put in place financial counselling, enduring powers of attorney, wills and advance care directives.
- Victoria Police can conduct welfare checks at the request of service providers. They can also provide support relating to financial abuse.
Recognising common perpetrator presentations and narratives
Any behaviour that is recognised as a family violence risk factor can be perpetrated against an older person.
The most commonly identified and visible form of elder abuse is the perpetration of financial abuse.
This may stem from the perpetrator’s ageist beliefs or attitudes (linked to the devaluing of older people in society). The perpetrator may also have a self-perceived entitlement to the older person’s resources, placing their own needs or desires above the needs of the older person.
Perpetrators often use psychological or emotional abuse to enact the financial abuse.
Some perpetrators use family violence in the form of neglect, such as intentional acts or omissions of care from family members who are responsible for care, including under guardianship arrangements.
People who perpetrate elder abuse may exhibit some of the following behaviours or narratives:
- Perpetrators may exploit or exacerbate actual or perceived ‘vulnerabilities’ to isolate and control the older person. This may include an adult child perpetrator leveraging a stereotype about older women and their capacity to manage finances in order to take control of decision-making, which is presented as ‘helping out’.
- Perpetrators may use community perceptions about their own virtue as a ‘carer’, their competence and worthiness, to present themselves to services as trustworthy, and to undermine a victim survivor’s confidence. They may undermine the victim survivor’s efforts to access system supports, such as health and aged care services, or not support or prevent them from independently accessing services. Sometimes, a perpetrator will purport to be a carer (and claim associated payments and/or accommodation) but not undertake any caring responsibilities.
- People who have caring responsibilities may seek to justify or attribute their use of family violence to ‘carer stress’, feeling that their caring work means they are entitled to additional control over the person they are caring for.[111] They may also seek to justify the violence because of perceptions of ‘sacrifice’ due to taking on caring responsibilities. Some people who use justifications of ‘carer stress’ may also resent their responsibilities and the older person, which can influence their self-perceptions about their use of violence (minimising their violence or blaming the person they are caring for). Ageism and perceptions about providing care and support for older people can contribute to the perception that certain behaviours are 'helpful' or inherent to the caring role, which in other contexts would be considered 'controlling'.
- A perpetrator might exploit stereotypes of older people being less competent than younger people and less able to make decisions for themselves as a way to justify controlling an older person’s access to communication, mobility or medical needs.
- A perpetrator may undermine the victim survivor’s cognitive functioning and play upon community perceptions of perceived vulnerability to justify control.
- A perpetrator may exclude the victim survivor from being present in hearings or major decisions about their lives by saying ‘they would be upset’ if they were involved.
Service access and engagement barriers for perpetrators
Perpetrators of elder abuse who are adult children or carers will have varying types of contact or engagement with the service system overall. They present with different circumstances and psychosocial needs – which may relate to their use of family violence.
These issues can introduce barriers to help-seeking or access to services that would enhance their motivation or capacity for behaviour change.
This may include circumstances and psychosocial needs of the perpetrator, including:
- mental health or wellbeing
- drug and alcohol use
- financial instability and gambling
- unemployment
- housing instability
- social isolation.
Points of contact might be through the health advocacy service supporting the older person victim survivor. These might include general practitioners, nurses and other health professionals, NDIS or other disability supports, pharmacists, social clubs, and banking and financial institutions.
Older people who use family violence may experience difficulties in accessing and maintaining engagement with services due to feelings of shame or other health issues, for example, dementia and other behavioural or cognitive issues, and mobility restrictions.
Practice considerations enabling access for older people who are experiencing violence should be considered to enable access to services for older people who are using violence.
In addition to above engagement of adult children and carers, refer to the practice considerations for responding to older people experiencing family violence (elder abuse), as to how they may also assist you with engaging an older person using violence.
12.1.6 Family violence against people from culturally, linguistically and faith-diverse communities
There are some commonly experienced risk factors for people from culturally and linguistically diverse and faith communities.
These can include:
- perpetrators' use of threats relating to immigration, visa status and sponsorship as forms of isolation, controlling behaviours and forced dependence on the perpetrator. This can occur across all relationships and identities. For people from LGBTIQ communities, this may include perpetrators exploiting fears about persecution, discrimination or rejection from family for the victim survivor if they were forced to return to their country of origin. A person’s culture and immigration status might also affect their experiences of family violence and willingness to disclose the violence
- family networks supporting the perpetrator's use of violence or feeling it is justified. This might include those family networks also perpetrating violence towards the victim survivor (multiple or proxy perpetrators) or socially isolating them from community and culture for choosing to address it
- service access barriers relating to a lack of services’ understanding of the complexities of family violence for particular communities and faiths
- victim survivors sympathising with perpetrators because of difficulties they are facing, such as experiences of racism.
Service access and engagement barriers for victim survivors
People from culturally, linguistically and faith-diverse communities can experience systemic barriers to seeking support including those relating to the following:
- speaking no or limited English or having limited access to interpreters (which may be more pronounced in rural and regional areas)
- limited access to information about family violence and support services, particularly in their preferred language
- limited information about Australian laws and services
- reservations about engaging with authorities or services due to past experiences or current fears and misconceptions. You can address these fears by providing support to understand why questions are being asked about their personal life and about their children’s safety, stability and development. You should spend time explaining how the system works in ways that are relevant to the person
- lack of cultural awareness and safety from service providers.
Practice considerations
Practice considerations for responding to people experiencing family violence from diverse cultural, linguistic or faith backgrounds, including people from migrant or refugee backgrounds, include, but are not limited to the following:
- Consider the cultural context of the person or family and how this may affect their experience of family violence. For example, the person may:
- face cultural stigma, taboos and social and community pressures
- be isolated from social or family networks as a result of family violence, particularly where they are newly arrived migrants, and may be dependent on partners or family members for financial support and transport
- have cultural or faith-based beliefs that discourage separation or divorce
- hold parenting norms and practices that are influenced by many factors, including culture and faith-based beliefs.
- Consider the effects of recent experiences of racism and discrimination in Australia (this extends to their children and other family members).
- Consider experiences of significant trauma prior to migrating to Australia, particularly where they are from refugee or asylum seeker backgrounds.
- Be aware of how visa or immigration status can impact on access to services. For example, they may be living in Australia on a temporary or provisional visa and fear the implications of visas being cancelled if family violence is disclosed. This fear can also extend to access to their children, where their children are Australian citizens, or where the perpetrator makes threats to take the children overseas. They may also fear facing punishment or being killed if they return to their country of origin. Perpetrators may exploit these fears.
- Be aware of fears about engaging the legal system or police. This may be due to lack of trust based on experience in their country of origin (if applicable), or because they have experienced or heard about others in their community experiencing racism from Australian police or legal systems. Some may also have particular fears and misconceptions about engaging with legal systems in Australia relating to residency and citizenship status.
Recognising common perpetrator presentations and narratives
While there are common narratives and presentations across all cohorts of people who use family violence, some nuances around beliefs and attitudes exist for people who use family violence from culturally, linguistically and faith-diverse communities.
These can relate to gender and family roles, relationships to extended family, responsibility for financial control and entitlement, dowry entitlement, parenting, visa access and stability, and age-related expectations.
Culture or religion should never be accepted as justifications for a person’s violence towards family members.
Perpetrators can feel protected by the community and community leaders, including at times where they feel their beliefs or attitudes about gender and family roles and acceptable behaviours are shared or colluded with, or pressure is placed on victim survivors not to report violence.
Service access and engagement barriers for perpetrators
When working with people who use family violence from culturally, linguistically and faith-diverse communities, you should seek to understand the varying and diverse cultural and spiritual dynamics in which family violence occurs.
Factors that may compound a perpetrator’s risk of using violence include:
- beliefs and expectations around family, family life and roles
- dynamics of perpetration by multiple family members, including extended family and in-laws in Australia or overseas
- the experiences of trauma associated with migration and asylum seeking
- experiences of racism, social isolation and distress related to immigration
- lack of access to formal and structural supports due to lack of culturally response services and visa status.
Some people experience increased barriers to accessing support around the use of violence.
As for all people who use family violence, the experience of shame impairs decisions for help-seeking, particularly from leaders within their own community.
Consider ways to enable access to services for victim survivors from culturally, linguistically and faith-diverse communities. Enabling service access by reducing barriers and structural inequality is also essential when working with people using violence from the community.
If working with a person using violence who is not from a culturally, linguistically or faith-diverse community, refer to guidance about service access barriers, as appropriate to the person’s identity, throughout this section.
People using violence who are from white, dominant culture backgrounds may present with specific tactics that invite collusion from professionals and exploit their privilege to ‘make invisible’ their own violence.
Where you recognise these tactics and behaviours, it is important to respond using a balanced approach to keep the person engaged with the service system (refer to perpetrator-focused Responsibility 3).
Identify opportunities to work collaboratively with other professionals to minimise further systems abuse and exploitation.
12.1.7 Family violence in lesbian, gay, bisexual, transgender, intersex and queer (LGBTIQ) communities
The majority of experiences of family violence among LGBTIQ communities mirror those within heterosexual and cisgendered relationships.
The impact of biphobia, homophobia, transphobia, heterosexism and heteronormativity on the experience and response to intimate partner violence in LGBTIQ relationships is pronounced.[112]
Heteronormativity is the internalisation of heterosexism at the individual, cultural and institutional level, as well as expectations about gender and sexuality, and their presentation in LGBTIQ relationships.
These forms of discrimination can also be used by LGBTIQ people to exercise power and control in their relationships.
Additionally, some LGBTIQ people may not recognise their experience as family violence. This is because it is primarily recognised across the community as experienced by cisgender women and children from cisgender men, and LGBTIQ people’s experiences fall outside of this traditionally recognised power dynamic.
While awareness of family violence in LGBTIQ relationships and communities is mixed, evidence suggests higher identification and self-reporting when presented with specific forms of violence experienced from an intimate partner or a family member rather than in general terms.[113]
A 2018 Our Watch literature review found that:[114]
- rates of intimate partner violence (IPV) against LGBTIQ people are as high as the rates experienced by cisgender women in intimate heterosexual relationships. However, rates of IPV may be higher for bisexual, transgender and gender-diverse people
- lesbians are more likely than gay men to report having been in an abusive relationship
- it is unknown how rates of IPV and/or family violence against people with intersex variations compare due to a lack of research
- violence from other family members may also be higher. Some examples are:
- young people subject to homo/bi/transphobia being kicked out of the home after coming out about their sexuality or gender identity
- gender diverse LGBTIQ people who rely on others for care and support because of age or disability having their means of gender affirmation denied, such as through the withholding of hormones by their children
- older, dependent transgender people being denied access to hormone treatment by their children.
The 2020 Private Lives 3 survey further indicates that, among participants:[115]
- more than 4 in 10 people identified ever being in an intimate relationship where they felt they were abused in some way, with emotional abuse, verbal abuse, physical violence and sexual assault commonly reported experiences
- almost 4 in 10 people identified ever feeling abused by a family member (either birth or chosen family), with verbal abuse, LGBTIQ-related abuse, emotional abuse and physical violence commonly reported experiences
- non-binary participants and trans men experienced higher rates of intimate partner violence and violence from a family member than cisgender women, cisgender men and trans women
- more than half reported the perpetrator of intimate partner violence to be ‘cisgender man’, and in reports of family violence almost three-quarters identified the perpetrator as ‘parent’
- while only 1 in 10 people reported LGBTIQ-related abuse from an intimate partner (e.g., threatening to ‘out’ the victim survivor, withholding hormones or medication), experiences of violence from family members was reported by survey participants as significantly linked to sexual orientation, gender identity and/or gender expression or intersex variation/s.
There are a number of family violence risk behaviours that are unique to intimate partner violence in LGBTIQ relationships. These include:
- threats to out, or actual outing of the partner, when they have not disclosed their sexuality, gender, intersex or HIV status, as a method of control
- threats to a partner’s capacity or right to children. This may be undermining or exacerbating fears about the legal status of children in same-gender relationships
- threats to limit or refuse a relationship with their children if they leave the relationship, when the other person is a non-birth or non-biological parent
- isolating the partner from contact with the LGBTIQ community and organisations, making it difficult for the abused partner to seek help, including using the victim’s intersex status, sexuality, transgender, gender expression or HIV status to threaten, undermine or isolate them from their family or community
- abusive and undermining gendering or misgendering in relationships, such as those relating to binaries of masculinity/femininity ‘butch’/’femme’
- exploiting deep feelings of unworthiness or shame the victim survivor might hold about being ‘deserving’ of the violence linked to experiences of discrimination, violence, and internalised biphobia, homophobia and transphobia
- controlling their partner’s access to health treatments and medications (such as access to hormone therapy for people transitioning to affirm their gender identity)
- if the perpetrator has a chronic illness, using guilt to manipulate or keep the partner in the relationship; threatening to, or actually infecting their partner where the illness is one that can be transmitted; deliberately placing their partner of significant risk by not taking reasonable precautions to prevent transmission
- using technology to facilitate sexual violence and harassment.
Service access and engagement barriers for victim survivors
LGBTIQ people may mistrust the service system due to previous experiences of historical institutional or interpersonal abuse, discrimination or uneducated responses.
There are a range of ways barriers to access and engagement present, including:
- avoiding services or only seeking them out during times of crisis for fear of further stigmatisation
- not reporting violence to police
- preferring to access LGBTIQ services rather than mainstream services
- seeking support through the community rather than the service system
- fear of revealing sexual orientation, intersex status, sex or gender identity to a service, leading to inappropriate responses
- poor levels of understanding by mainstream service providers of key issues including common patterns of violence against LGBTIQ people, and how to respond/refer. Examples of myths include:
- that the more masculine partner is the more violent
- that women cannot be violent
- that biological parents have a more significant connection with children. This can lead to risk being underestimated, violence minimised and/or the victim not being believed or responded to
- the lack of crisis services for male, transgender and non-binary victim survivors (particularly crisis accommodation), and programs for female and non-binary perpetrators
- a limited understanding of homo/bi/transphobia from family of origin as being recognised as family violence and appropriate referral pathways.
The number of LGBTIQ family violence services is limited.
However, it has expanded since the Royal Commission, and the family violence sector as a whole is building knowledge and capacity around LGBTIQ family violence inclusion in mainstream services.
Practice considerations
Practice considerations for responding to LGBTIQ people experiencing family violence include, but are not limited to the following:
- Recognise how the dominant understanding of family violence as only involving heterosexual cisgendered male perpetrators and their cisgendered female partners contributes to low levels of identification and reporting and is a key factor in the ‘invisibility’ of family violence against LGBTIQ people.
- Be mindful of the diversity of identities and experiences across ‘LGBTIQ’ to consider the individual’s specific identity and what this means for risk assessment and management.
- LGBTIQ people may fear isolation or losing community support or connections by reporting family violence, particularly as they may have less support from their family of origin.
- There may be pressure not to identify violence or abuse within LGBTIQ relationships for fear it may fuel homo/bi/transphobia — particularly following the high levels of homo/bi/transphobia against LGBTIQ people during the 2017 Marriage Equality debate.
- Consider current and historical discriminatory laws against people on the basis of sex, sexuality and gender identity (among other attributes), such as where they conflict with religious beliefs, contributing to fears of discrimination from services.
- Be mindful of failing to recognise LGBTIQ victim survivors’ identity or relationships, for example providing personal safety intervention orders instead of family violence intervention orders.
- Children and young people who experience family violence are more likely to suicide at all points along the journey from seeking safety to recovery and health. The risks of suicide are extremely high in young LGBTIQ people, particularly trans and gender-diverse young people. For LGBTIQ young people, this additional high risk is compounded by an increased risk if they have experienced family violence.[116]
Recognising common perpetrator presentations and narratives
Many stereotypes exist about LGBTIQ intimate partner violence. These can both influence professionals’ responses and form the basis of narratives provided by perpetrators to minimise or justify their behaviour.
In the context of relationships across LGBTIQ communities, cisnormativity, heteronormativity, and social norms and understandings around gender and sexuality can be internalised and imported into LGBTIQ relationships, leading to particular forms of coercive and controlling behaviours.
While similar patterns of coercive and controlling behaviour occur, heterosexist attitudes can also play out within LGBTIQ relationships along masculine and feminine relationship dynamics.
The general tolerance of violent expressions between heterosexual cisgender men within society has provided the foundation for normalising abuse, as well as making invisible the real prevalence, seriousness and impact of risk associated with family violence in relationships between male-identifying people, which is often not ‘seen’ or is downplayed.
There may be an assumption that only straight, cisgendered men are violent. Similarly, where there is violence between cisgender women or female-identifying people, this may not be visible or may be downplayed as ‘less serious’ or perceived as less likely/believed than violence between cisgender men.
Common presentations of behaviours and narratives among perpetrators include:
- the violence is a result of ‘mutual violence’
- the violence is ok because ‘men fight equally’, ‘boys are being boys’ and have comparable strength
- violence doesn’t occur in female-identifying same-gender relationships, presenting the belief or narrative that violence is only perpetrated by cis-men
- avoiding responsibility for violence through using chronic illness and ‘weakness’ to deflect the possibility that they could be abusive or controlling
- claiming the other person is a perpetrator of violence based on their physical stature or physical conformity to heteronormative expressions of gender and sexuality
- expressing previous experiences of trauma as anxiety to justify control over a current partner
- outing them to family, community networks, employers etc.
Guidance on responding to narratives of ‘mutual violence’ is outlined under guidance on identifying predominant aggressors in Section 12.2.1, and in the victim and perpetrator-focused Responsibilities 3, 5, 6 and 7.
Service access and engagement barriers for perpetrators
The same practice considerations for enabling access to services for LGBTIQ victim survivors apply for perpetrators.
In engaging or working with people from LGBTIQ communities who are using family violence, you should understand how multiple layers of discrimination, stigma, marginalisation and oppression are experienced and perpetuated through systems and services. In your practice, you should seek to work against these factors.
Key considerations for working with people using family violence include the following:
- Remove barriers leading to stress and the reduction of help-seeking (e.g., housing).
- Understand the dual nature of victimisation and perpetration of violence experienced by this community.
- Use inclusive language
- Understand the broader issues faced by LGBTIQ people, without affirming stereotypes.
12.1.8 Family violence against LGBTIQ people by families of origin
Family violence against LGBTIQ people by family members is widely unrecognised across the service system.
Recognising common family of origin perpetrator presentations and narratives
This form of family violence may present in a range of ways, including:
- undermining sexual orientation or gender identity and the value of intimate relationships, calling it a ‘phase’ or not a real relationship
- refusing to acknowledge the status of the relationship or the partner by ignoring them
- refusal to use or correcting their pronouns (including the pronouns of their partner)
- using beliefs about faith or religion, gender, sexuality, family and relationships to de-legitimise or undermine identity of an LGBTIQ person, particularly young people. This could lead to relationship breakdown, housing and financial distress and parental/family abandonment
- minimising or justifying violence and harm under the guise of ‘protective parenting’ or ‘rights’ to parental control and discipline, rather than as family violence and targeted harm that is based on their child’s sexual orientation or gender identity (also refer to perpetrator-focused Responsibility 2– observable narratives and behaviours).
Note that coercive and controlling behaviours including pressure to participate in conversion practices and services. These are recognised examples of family violence under the Family Violence Protection Act 2008 and of harassment under the Personal Safety Intervention Orders Act 2010.
Service access and engagement barriers for perpetrators
In engaging or working with family of origin who are using violence, it is important to keep the following in mind:
- Often violence from family members related to identity and relationship recognition is not seen as family violence, making it harder to raise awareness and link to behaviour change supports.
- Some barriers to service engagement are related to minimising and justifying in relation to beliefs in ‘rights’ of parental control and discipline. These narratives may legitimise biphobia, homophobia or transphobia based on personal and faith-based beliefs not held by the victim survivor. For example, this includes a parent’s belief in their ‘legitimate’ right to object to their child’s sexual orientation or gender identity.
People using violence who are not from LGBTIQ community may present with specific tactics that invite collusion from professionals and exploit their privilege to ‘make invisible’ their own violence.
Where you recognise these tactics and behaviours, it is important to respond using a balanced approach to keep the person/family engaged with the service system (refer to perpetrator-focused Responsibility 3). This includes identifying opportunities to work collaboratively with other professionals to minimise systems abuse, exploitation and further violence.
12.1.9 Family violence against people with disabilities
There are more than one million people with a disability living in Victoria.[117] This includes a wide range of disabilities that can affect how people access and participate in services, family and community in different ways.
Disabilities can be cognitive, physical, sensory, result from acquired brain injury, be neurological, or related to mental illness.
Further information about the relationship between family violence and acquired brain injury can be found in the ‘Acquired brain injury as a result of family violence’ section below. Section 12.1.10 discusses family violence and mental illness. Section 12.1.17 discusses perpetrators with complex needs, including cognitive disability and acquired brain injury.
Family violence is the leading cause of death, disability and ill health in women aged 18–44.[118] People of all genders with disabilities are also at higher risk of experiencing family violence.
The intersection of gender and disability increases the risk of violence against women and girls with disabilities.[119] International and Australian evidence shows that women with a disability experience violence more intensely and frequently than other women.[120]
The Victorian Royal Commission into Family Violence acknowledged women with disabilities experience all forms of violence at higher rates than women without disabilities.
People with disabilities are also affected by current and historical practices of institutionalisation, and trauma stemming from this needs to be considered, along with any barriers they may present to future services engagement.
The social model of disability can help you respond to marginalisation and discrimination. This model recognises that disability is not only a person’s condition, but the result of disabling social structures, attitudes and environments.[121]
You should have a general awareness of different types of disability and ask people with disability about any support requirements or adjustments they need.[122]
Service access and barriers for victim survivors
People with disabilities may face several barriers affecting their ability to seek support including:
- lack of economic resources and/or sufficient income
- lack of support options (or lack of awareness regarding support options)
- lack of access to refuges and other suitable long-term housing alternatives
- lack of access to interpreters, communication devices, assistance to communicate and information in an appropriate format
- bias of professionals in their recognition or engagement with people with disabilities.
Specific barriers to receiving appropriate and effective services include services lacking knowledge and confidence in working with people with disabilities, and professionals believing they are ill-equipped to respond.
Professionals can address this by working in a proactive and collaborative way, including through secondary consultation and referral with organisations specialising in working with people with disabilities (refer to victim survivor–focused Responsibilities 5 and 6).
People with disabilities experience barriers that arise from particular dynamics and forms of family violence, which among other things can affect a willingness to disclose family violence. These can include the following:
- People with disabilities may be reluctant to report the violence because the perpetrator may be controlling or isolating them through their assistance with essential activities, such as personal care, communication, mobility, parenting or transport.
- Perpetrators might use particular tactics towards victim survivors with a disability to exploit and exacerbate general fears relating to experiences of discrimination in the community. This might include threatening victim survivors with being sent to institutions or support services as a way of undermining both the victim survivor and their relationships with children.
- Some people with disabilities may normalise the experience of being controlled and abused, especially if this has been accepted by service providers. For example, where a carer is asked or encouraged to ‘speak for’ the person with the disability.
- People with disabilities can experience social isolation stemming from the marginalised position of people with disability in society.
- Professionals should be aware of issues relating to failure to address family violence perpetrated in a community residential or other care settings (for example, where a resident uses violence against another, or a long-standing carer in a ‘family-like’ relationship uses violence against a person with disability).
- People with disabilities can be the subject of negative stereotypes or discrimination, which can mean people are not believed when they report violence and tailoring your approach to reassure the person against these assumptions and stereotypes. These stereotypes can impact:
- perceptions of their capability as parents
- perceptions of the likelihood of the person lying or misunderstanding situations as violent
- perceptions of their capacity to provide evidence, including competent testimony in court
- increased risk of having their child removed from their care for parents with a disability, or experiencing a mental health issue, homelessness or who live in a regional area.[123]
For example:
- Women with disabilities are often undermined about their parenting skills and abilities as a common tactic used by perpetrators, which can be reinforced through conscious or unconscious bias by professionals.
- Women with children with disabilities can experience additional barriers to service or risk management responses where there is lack of ‘responsibility’ taken by services in providing coordinated responses.
- Children with disabilities may not have their experience of risk from a perpetrator’s behaviour adequately identified or assessed, including behaviours that are targeted directly to them or indirectly by witnessing or being exposed to its impacts, particularly on their caregivers.
- Women with disabilities have commonly experienced discrimination, structural inequality (including in the form of physical and communication barriers) and bias when seeking to access services.
- Women with disabilities may experience lifetimes of discrimination and violence, preventing them from opportunities to experience safety and make free choices.
Practice considerations
Practice considerations for responding toand attempting to overcome these barriers for people with disabilities experiencing family violence include, but are not limited to the following:
- Use a respectful, strengths-based approach. Believe the person and take their experiences seriously. While this is important for all victim survivors, it can be particularly important for people with disabilities in the context of these barriers, fears, assumptions and stereotypes.
- Recognise how experiences of marginalisation and discrimination might affect the person’s engagement. Address any physical or communication access barriers. Person-centred responses that adjust the environment to fit the needs of a person with intellectual or other cognitive disabilities will improve the person’s capacities to respond to the demands of the context.[124] This includes providing access to communication supports and adjustments if needed, such as Auslan interpreters for people who are Deaf or hard of hearing, communication aids and accessible formats.
- Ensure responses are guided by principles and obligations under the Medical Treatment Planning and Decisions Act 2006 (Vic) and Guardianship and Administration Act 1986 (Vic) when working with people with a disability or whose cognitive capacity is affected.
- Some people with disabilities may have a guardian or administrator. The guardian must act as an advocate for the person, act in their best interests, take into account their views and wishes and make decisions that are the least restrictive of the person’s freedom of decision and action.[125]
- Design interventions to provide support to enable people with cognitive disability to participate in services. Such interventions and supports include issues pertaining to Universal Design for Learning, multi-tiered systems of supports, and promoting the self-determination of people with disabilities.[126]
Acquired brain injury as a result of family violence
Acquired brain injury (ABI) can result from a perpetrator’s use of external force applied to the head (including with weapons, striking the head, shaking or being pushed into an object or to the ground) and from stroke, lack of oxygen (including from choking or strangulation) and poisoning.
ABI can result in a range of physical, cognitive and behavioural disabilities that can impact adults, children and young people in a variety of ways, including their capacity to engage in safety planning and risk management.
Recent Victorian research found that the association between family violence and ABI in Victoria is significant.[127]
It is likely to be more significant even than this research suggests, as this data is unlikely to reflect all cases of ABI.
Most victim survivors will not seek medical attention or attend a hospital when they have sustained a brain injury as a result of a perpetrator’s actions. Even if they do, their brain injury may not be detected.
This includes childhood head injuries that may never have been attended to, resulting in long-term impacts.
Aboriginal women are at very high risk of traumatic brain injury, with research suggesting they are 69 times more likely to be hospitalised for head injury due to assault.[128]
Children are more vulnerable to brain injury from physical assault because of their smaller size and rapidly developing brains. Inflicted brain injury (which includes ‘shaken baby syndrome’) is the leading cause of death and disability in children who have been abused. Infants are at the greatest risk.
It is important to remember that victim survivors may be concerned about the stigma of disclosing ABI concerns. In particular, they may fear that this could lead to questions about their personal agency or autonomy, decision-making and parenting capacity.
You should also be sensitive to the concerns that victim survivors may have if they had not previously understood the impacts of violence on the brain, for themselves and their children.
Victim survivors may also find the possibility of being diagnosed with an ABI confronting, especially if they have not previously identified as a person with disabilities.
Perpetrators may also have ABIs, as a result of experiences of violence, including family violence.
This can affect their response to interventions or risk management strategies, so it is important to consider this possibility during risk assessment.
Recognising common perpetrator presentations and narratives
An intimate partner, carer, adult child or other family member may be using family violence against a victim survivor with disability.
They may target perceived ‘vulnerabilities’ or use ableist beliefs to weaponise the structural inequality, barriers or discrimination experienced by the victim survivor.
A person using violence may use these tactics as a way to methodically gain power and control over the victim survivor and avoid taking responsibility for their use of violence.
Stereotypes about disability can form the basis of narratives provided by perpetrators to minimise or justify their family violence behaviour.
These ableist stereotypes and beliefs can also affect professionals’ responses to people with disability, through colluding with the narrative of the person using violence.
Common presentations of family violence behaviours and narratives among people who use violence against people with disability include:
- exploiting community attitudes of carers being ‘virtuous’ and ‘helpful’ as a tactic of system collusion, undermining the victim survivor’s involvement in the service. They may present to the service in a way that the professional believes the victim survivor is ‘lucky’ to have them in their life. Similarly, the perpetrator may blame ‘carer stress’ as a way to avoid taking responsibility for their actions or behaviours, or minimise their violence or its impacts on the victim survivor
- undermining or pathologising a person’s cognitive capacity, for example, through statements such as, ‘They’re crazy, you need to speak with me because they don’t understand things.’
- weaponising community assumptions about people with disabilities as parents and threatening to institutionalise the victim survivor, and/or to have the victim survivors’ children removed
- withholding food, water, medication or personal care, or threatening to do so, to coerce and/or control the victim survivor
- tampering with the victim survivor’s support devices (e.g., removing parts of a wheelchair) to further exert control.
It is important to be aware that people using violence will target a victim survivor’s specific disabilities.
People who use violence who are carers may also exploit confusion around navigating support systems such as the NDIS or Centrelink to maintain control as ‘gatekeepers’ to service access.
This type of behaviour can manifest in a variety of ways.
For example, the person using violence might:
- be the NDIS nominee and exploit this to make decisions for the person with disability, isolating them from support and misuse their finances
- reinforce or exploit the victim survivor’s fear of using disability services, perpetuating a narrative that interventions will subject them to discrimination and harmful stereotyping
- present to services with the victim survivor and answer on their behalf and not allow the victim survivor to respond
- constantly express dissatisfaction with services or carers who are sent to provide in-home care. This constant dismissal of services could be another tactic of isolating the victim survivor and maintaining control.
This ‘gatekeeping’ of service access can lead to system collusion. You should be aware of the presentations and narratives you observe and respond to them as family violence risk to the victim survivor with disability.
Service access and barriers for perpetrators
People who use family violence towards people with disabilities are most likely to be identified through their engagement with the service system on behalf of a person with disability.
When you recognise narratives and invitations to collude, you can seek to engage with the person/carer using violence by drawing out information about their perception of their carer role.
A person using violence who is in a caring role may have additional ‘barriers’ to engagement, such as stoicism, inability or reluctance to accept alternative options for care, and beliefs about the role of family in the person’s care (rather than services).
Opportunities to reduce barriers to service access for both themselves and the person with disability may present through processes of reframing caring responsibilities to include other supports available.
Practice considerations enabling access for victim survivors with disabilities should be considered to enable access to services for people using violence with disabilities.
If working with a person using violence against a person with disability, refer to guidance about service access barriers, as appropriate to the person’s identity and relationship to the victim survivor, described throughout Section 12.1.9.
People without disabilities who are using violence may present with specific tactics that invite collusion from professionals and exploit their privilege to ‘make invisible’ their own violence.
Where you recognise these tactics and behaviours, respond using a balanced approach to keep the person engaged with the service system (refer to perpetrator-focused Responsibility 3). Identify opportunities to work collaboratively with other professionals to minimise opportunities for systems abuse, exploitation and further violence.
Section 12.1.17 outlines recognition of perpetrators of family violence with cognitive disabilities, including ABI.
12.1.10 Family violence against people with mental health issues and mental illness
People with mental health issues and mental illness and psychological distress experience particular barriers and forms of family violence.
A perpetrator’s use of family violence can exacerbate existing mental illness, cause mental disorder and mental illness, and impact negatively on recovery.
Perpetrators may be carers who are intimate partners, parents, children or other family members or carers who have a family-like relationship to the victim survivor.
The main mental health impacts of family violence are anxiety, depression and suicidal ideation.
Eating disorders, problematic alcohol and drug use as a coping mechanism, postnatal depression, self-harm, post-traumatic stress or Post Traumatic Stress Disorder and suicide are also associated with family violence.
High rates of mental health issues and mental illness following family violence demonstrate the need for support that takes these mental health impacts into account.
Many victim survivors, especially women, experience family violence following a mental illness diagnosis.
Perpetrators can use this perceived vulnerability to target women with mental illness, resulting in their experience of multiple forms of violence that lead to greater mental health impacts.
The more recent and the longer the violence has occurred, the greater the mental health impacts. The same has been found for childhood (sexual) abuse and its short to long-term impact.
Prevalence rates of any form of abuse for people who access psychiatric services are high — between 30–60 per cent of people have a history of family violence and 50–60 per cent have experienced childhood sexual or physical abuse.[129]
Some studies have found that up to 92 per cent of female psychiatric inpatients have histories of childhood abuse, family violence or both.[130]
People, especially women, experiencing psychosis, schizophrenia, bipolar disorder and borderline personality disorder have experienced high levels of abuse.[131]
Many people with a diagnosed mental illness have experienced both childhood abuse and family violence as an adult.
Women who have also experienced childhood trauma are more likely to experience depression for a longer time, pointing to the cumulative effect of multiple traumas.
Women who have experienced severe abuse are more likely to be diagnosed with one or more mental illnesses in their lifetime. Levels and severity of depression tend to decline over time as women feel safer.
Women accessing family violence support services, especially crisis services, experience high levels of mental health issues, including anxiety (at rates three times higher than the general population) and depression (twice that of the general population).
In Victoria, one-third of people who die by suicide had a history of family violence.
Family violence had been present for half of the women (identified as likely victim survivors) and one-third of men who died by suicide (identified as likely perpetrators).
Further, as noted in Section 12.1.15, threats or attempts to self-harm or commit suicide are a risk factor for homicide–suicide.[132] This factor is an extreme extension of controlling behaviours.
Practice considerations
Practice consideration for responding to people experiencing family violence who have mental health issues or mental illness include, but are not limited to:
- Experiences of significant stigma and discrimination can have a worse impact than the mental illness itself.
- People with mental health issues and mental illness, particularly women, and their family members are at greater risk of being isolated from support networks and lack of adequate support by organisations, including mental health and family violence services.
- People with mental health issues and mental illness, particularly women, are more likely to disclose family violence to a healthcare professional than the police, and they are unlikely to do so unless they are asked. At the same time, many people with mental illness or mental health issues, particularly women, report problematic responses by professionals following disclosure. Inadequate support can increase distress and leave people with mental illness or mental health issues in unsafe situations.
- People with mental health issues may be at higher risk of sexual assault and may not be believed if they report abuse.
Barriers to accessing support from the service system include:
- People with a mental illness may not be believed by professionals, especially if they experience psychosis or psychotic illnesses, or professionals might judge them as untrustworthy in their account or narrative of their experience.
- Perpetrators may use a mental health diagnosis to ‘gaslight’ a victim survivor, meaning that they may not easily recognise the violence they have experienced, or may struggle to feel entitled to accessing services.
- Service providers who are not mental health services lack confidence and consider themselves poorly equipped to work with a person with a mental health issue or mental illness.
- Organisations having a narrow understanding of their role. For example, mental health services have historically not embraced their role working with victims of family violence.
- A lack of understanding of the links between trauma and mental illness by the service system. The dominance of the bio-medical model means that trauma and mental illness are frequently separated, and distress is pathologised as mental illness, rather than a normal reaction to trauma.
- Service providers may not understand how trauma manifests, for example, through anxiety or depression, and may be influenced by stigmatised views of mental illness.
- Service providers may misunderstand a victim survivor’s distress and pathologise a normal reaction to violence as mental illness.
- People with multiple presenting needs, such as a mental illness and alcohol or drug issues, are more likely to experience barriers to service responses unless professionals are well linked and understand the interrelated nature of their presenting needs.
Section 12.1.17 provides guidance on perpetrators with complex needs, including mental illness.
12.1.11 Adolescents who use family violence
This section provides guidance on the presentation of and high-level response to adolescent family violence.
The victim survivor–focused MARAM Practice Guides emphasise that adolescents who use violence are also likely victim survivors who should be assessed and supported with risk management responses.
Adolescents who are using violence should have a different response from adult perpetrators.
The adolescents using violence MARAM Practice Guides provide more information. These also address adolescents who use violence who have disability or cognitive impairment.
Most incidents of violence are committed by male adolescents against mothers, which may progress to using violence against women as adults.[133]
Violence in the home from an adolescent towards a sibling is a specific form of violence.
There is evidence that sexually abusive behaviours by adolescents is more often directed towards younger siblings.
The most common type of sibling sexual abuse is between a brother and a sister, with the brother as the abusing sibling, and brother towards brother sexual abuse is the second most common form.
Children who display problematic sexual behaviours towards their siblings may be acting out trauma as a result of having been sexually abused themselves.[134]
Responses to children and young people should consider their age and developmental status, attachment and relational history, their strengths and protective factors, their care situation and their overall context. This includes whether they have experienced or are currently experiencing family violence.
Responses to sexually abusive behaviours requires a specific and targeted response that should include sexually abusive behaviours treatment services.
When working with adolescents who use violence, avoid labelling them as ‘violent’ or ‘perpetrators’. This can lead to them internalising these labels, and it can also make it harder for you to recognise their behaviour as part of a trauma response or to use a relational trauma lens supporting behaviour change.
At the same time, you should provide clear and consistent messaging that violence is not acceptable and support them to take responsibility for and change their behaviour.
When assessing a victim survivor’s level of risk, guidance outlined here relating to working with perpetrators may also be applicable to considering the impacts of violence by an adolescent on a victim survivor.
Violence by an adolescent against a parent/carer may result from an impact of trauma, for example the inability to process emotions, self-soothe and deal with conflict.
Nevertheless, an important learning for an adolescent recovering from the impact of trauma is to be accountable for the use of violence and to learn skills and abilities to move away from the use of violence.
Having a trauma-informed approach can be held at the same time as working with an adolescent to be accountable. This is important for the adolescent’s own development and to ensure others who are in close relationships with the adolescent are safe. This work is done with respect, and in a sensitive non-blaming manner.
Professionals working with adolescents need to be mindful of collusion.
This is particularly relevant if a professional is working with an adolescent without the presence or input of a parent/carer.
Adolescents, like adults who use family violence, may minimise their use of violence and its impacts, justify and deny their use of violence and blame others, particularly parents/carers for ‘causing’ them to use violence.
You need to be able to challenge these constraints to taking responsibility and making change.
Collusion occurs when a professional sides with the adolescent against other family members or gives a message (even inadvertently) that the use of violence is understandable.
Collusion can occur where a professional over-identifies with an adolescent or their experience.
The adolescent may describe a picture of being the victim and provide convincing reasons for why they are unfairly being blamed for the violence. Professionals need to carefully assess the family dynamics and patterns so as not to over identify or collude with the adolescent.
Collusion can also occur with a parent/carer where the parent/carer has been abusive or violent to the adolescent.
A parent/carer may describe an adolescent’s behaviour in a way that does not account for family history, experience and dynamics.
Careful assessment to fully understand the family patterns and dynamics is important so as not to collude with any family members using abuse or violence.
Working with adolescent family violence needs to be a ‘both/and’ approach. This means the adolescent may be living in a family context where parenting is abusive, they may have experienced family violence, or they may be dealing with complex and distressing life events and issues.
The professional needs to address these contexts as well as hold the line that violence is not acceptable.
In this context, professionals need to work with the adolescent to take responsibility for their use of violence, and to also work with other issues of concern.
Further guidance on working with adolescents as victim survivors is provided in the victim survivor–focused MARAM Practice Guides.
Young people aged 18 to 25 years should also be considered with a developmental lens and to ensure any therapeutic needs relevant to their age and developmental stage are met.
The adult perpetrator-focused MARAM Practice Guides include relevant information for working with young people aged 18 to 25 years who are using family violence to assess and manage their risk.
12.1.12 Family violence against men [135]
Family violence against male victims is significantly gendered . Most men experience family violence from other men, including across age groups, relationship types and communities.
In Australia, approximately 94 per cent of female victims of violence and 95 per cent of all male victims of violence report a male perpetrator.[136]
The gendered nature of family violence stems from the dominant gendered culture, which reflects structures of power and privilege as created and perpetuated by cisgender, white ‘masculine’ men.
Many men are influenced by dominant norms and expectations about masculinity, or ‘ways to be a man’.
They may measure themselves and others against stereotyped characteristics, such as suppression of emotion or, expression of aggression, dominance and control.
Dominant gendered culture plays out in various and complex ways across communities and relationships.
It drives norms and expectations in relationships and can shape the use of family violence by men towards other men in the family, or in same-gender relationships.
A smaller number of heterosexual, cisgender men do experience violence from cisgender female intimate partners.
Professionals should exercise caution when responding to family violence where this relationship dynamic is reported.
There may be potential for perpetrators and victim survivors to be misidentified where male perpetrators report or present as a victim survivor, adopting a victim stance.
Male perpetrators may adopt a victim stance generally, or in relation to their experience of violent resistance from a victim survivor.
Men who experience violent resistance from victim survivors (violence that responds to their own ongoing use of family violence risk behaviours, such as coercive and controlling behaviours) are not victim survivors.
Refer to Section 12.1.13 for further guidance on women who use force, and Section 12.2.1 on determining the perpetrator/predominant aggressor.
Non-specialist professionals should have some understanding that these issues might present and refer to specialist family violence services for comprehensive assessment where there is uncertainty about how to determine who is the victim survivor or the perpetrator/predominant aggressor.
For men who are determined through MARAM risk assessment to be a victim survivor, the victim survivor–focused MARAM Practice Guides are appropriate for use.
If they are determined to be the predominant aggressor/perpetrator, the perpetrator-focused MARAM Practice Guide is appropriate for use.
12.1.13 Women [137] who use force in heterosexual intimate partner relationships
There is no consistent prevalence data for cisgender women who use force in intimate relationships, either in Australia or internationally.[138]
Research suggests women who use force in heterosexual intimate partner relationships often have a history of experiencing family violence from their male partners.[139]
They tend to use force to gain short-term control over threatening situations, rather than using already held power to dominate or control their partner.
This motivation is distinctly different from men’s use of violence, which is characterised by a pattern of coercive, controlling and violent behaviour.
Women use force for a range of reasons, including to protect themselves and their children or in self-defence or violent resistance.
Where ‘mutual violence’ has been identified (that is, a woman has used force and their male partner is using family violence), violence is often asymmetrical, with men demonstrating stronger patterns of coercive controlling and violent family violence risk behaviours than women.[140]
In this context, women are often misidentified as a perpetrator/predominant aggressor.
This occurrence is reflected in the high rate of misidentification of women as perpetrators. For example, emerging evidence suggests that approximately 1 in 10 women named as respondents to police applications for family violence intervention orders are subsequently assessed to be victim survivors.[141]
Because of this, caution is required when working with cisgender women who are identified, at any point in the system, as perpetrators of family violence, particularly if:
- there are cross-accusations of violence between heterosexual cisgender people, and/or if a cisgender woman is identified as the person using violence towards a cisgender man
- a woman is identified as a respondent to a family violence incident.
Guidance on identifying the predominant aggressor is outlined in Section 12.2.1, and in the victim survivor and perpetrator-focused MARAM Practice Guides for Responsibilities 3, 5, 6 and 7.
You should use the victim survivor–focused MARAM Practice Guide when working with women who are determined through MARAM risk assessment to be a victim survivor.
If they are determined to be the predominant aggressor/perpetrator, the perpetrator-focused MARAM Practice Guide is appropriate for use.
12.1.14 Perpetrators’ experience of shame and use of externalised violence
Shame, as both an emotion and a process, occupies a challenging space for responding to people who use family violence.
Although Victoria’s system-wide response depends on holding perpetrators to account for their behaviour, confronting a perpetrator about their use of violence through ‘shaming’ processes can increase risk for victim survivors and result in further denial of responsibility.[142]
Studies have found that shame is often associated with increases in aggression and a tendency to hide away and externalise responsibility for socially unacceptable behaviours.[143]
While a perpetrator’s feelings of shame can maintain violent and coercive controlling behaviours and work as a barrier to help-seeking, addressing shame is a central aspect of specialist perpetrator intervention work towards change and personal accountability.
Not all professionals working with people using violence will address shame, however, it is important to be aware of its experience and consequences, and what it may mean for engagement and increased risk.
Shame may be compounded by gendered drivers, dominant culture and social norms such as masculinity. This may reinforce tendencies to externalise distress and blame and reduce the person’s capacity to take responsibility for their behaviour, to express themselves honestly and to seek help.[144]
When shame becomes toxic, people who use violence may experience reduced self-esteem and worth (for example, at the loss of a relationship with a partner or children).
A sense of hopelessness and worthlessness may become exacerbated, increasing the risk of harm towards self and violence towards others.
This can be identified as depression or reduced mental wellbeing for people at risk of suicide, which may also present as aggression/anger and violence towards adult (usually intimate partners) and child victim survivors.
Understanding the context and outcomes of shame assists in identifying the connections between the risk of self-harm and suicide with the risk of homicide or homicide-suicide.
Stigma associated with perpetrating violence is a barrier to help-seeking and engaging in services.
Feeling ‘judged’, ‘attacked’ or ‘threatened’ by services or programs is common, and so forming trusting and positive professional relationships is essential.
12.1.15 Suicide risk of adult perpetrators and adolescents using violence
Some risk factors for family violence are largely ‘in common’, or the same as those for risk of suicide for adult perpetrators and adolescents using violence.
The risk factors that are ‘in common’ are understood through the correlation of increased risk of suicide for adult perpetrators and young people using violence.[145]
Recognising increased risk of suicide of people who use violence
Between 2009 and 2012, around one-third of all suicide deaths of men in Victoria involved men with a history of interpersonal violence, of which more than half had been identified as perpetrators of violence. Some were also victim survivors of violence, usually as children.[146]
The National Homicide Monitoring Program has found that 80 per cent of homicide–suicides in Australia since 1989 occurred in the context of family violence.[147]
Homicide–suicides are most likely to be perpetrated by men who:
- are older
- exhibit paranoid thinking and depression
- use alcohol to harmful levels
- have histories of impulsivity and violence
- have prior suicide attempts
- extreme minimisation and/or denial of family violence perpetration history
- obsessive behaviour, including stalking
- prior forced physical confinement and restriction of movement
- experience despair and hopelessness.[148]
Despair and hopelessness are key indicators of escalated risk and the need for immediate risk management.
Responsibilities 3 and 4 have further guidance on identifying and responding to suicide risk.
There are many ‘in common’ risk factors for suicide and family violence, which reflects the high rates of family violence perpetrators in cohorts of people who die by suicide. These include alcohol or drug abuse, anger, reckless behaviour, and talking about death (threatening suicide).
Risk factors for suicide are outlined below, with factors in common with family violence indicated with the + symbol:
- previous suicide attempts
- history of substance abuse+
- history of mental health conditions+ –depression, anxiety, bipolar, PTSD
- relationship problems+ –often described as ‘conflict’ with parents and/or romantic partners, or separation
- legal or disciplinary problems
- access to harmful means, such as medication or weapons+
- recent death or suicide of a family member or a close friend
- ongoing exposure to bullying behaviour
- physical illness or disability.
Further guidance on identifying and understanding common risk factors between suicide and family violence risk is outlined in the perpetrator-focused MARAM Practice Guides for Responsibilities 3 and 7.
Indicators of serious and escalating risk among this cohort that must be acted upon immediately include:
- expressing feelings of losing control of the relationship, in particular, observing obsessive and desperate behaviours and victim-stance narratives
- losing connection with protective factors, such as employment, connections with social and other supports
- declining mental wellbeing and statements about inability to cope, expressions of feeling hopeless
- perpetrator narratives that empathise with other men who have killed partners or children, for example ‘I now understand what they went through when they killed their partner/child’.
Each of these indicators is linked to suicide and homicide–suicide risk.
Suicide risk among adolescents who use family violence
Adolescents who use family violence have unique suicide risk factors in addition to those experienced by adult perpetrators. This is compounded by increased risk of suicide for young people who have experienced family violence as victim survivors.
The 2019 Commissioner for Children and Young People report Lost, not forgotten identified that:
… as children grow older and their trauma starts to manifest in challenging behaviour, disengagement from school, risk taking, violence or mental ill health, professionals lose empathy. The children become seen as the problem and referred to as ‘difficult’, ‘needy’, ‘angry’ and ‘bad.’[149]
This report found that between 2007 and 2019:
- 94 per cent of children who were known to child protection (particularly repeat reports) and who died by suicide had experienced family violence, and most had parents with mental illness and/or substance use issues[150]
- 84 per cent were either diagnosed or suspected to have mental illness[151]
- 83 per cent were recorded as having engaged in deliberate self-harm[152]
- 51 per cent of the children who died by suicide in this period had contact with police in the 12 months before their deaths, 43 per cent within six weeks of death[153]
- of those who had police contact, 44 per cent were alleged to have used family violence against a family member.[154]
Practice considerations when identifying suicide risk
To date, assessment tools for assessing proximal suicide risk have been considered both ‘imperfect’ and ‘one of the most stressful tasks for clinicians’.[155]
Therefore, emerging suicide prevention research and practice places less emphasis on ‘risk assessment’, and more on identifying the drivers of suicidality and an individual’s intent.[156]
Professionals working with people who use violence are well placed to consider the ‘in common’ risk factors.
In family violence risk management practice with adult perpetrators and young people who are using violence, suicide safety planning, or a mental health referral response where the common risk factors are identified, is a standard minimum response across the service system and particularly for specialist practitioners.
Also consider referrals to manage social distresses that increase suicide risk, such as employment, financial and housing issues and drug and alcohol addition/use.
Common family violence and suicide risk factors, and protective factors, are considered under Responsibilities 3 and 7.
12.1.16 Family violence perpetration at the time of or following natural disasters and community-wide events
Emerging research highlights the links between prevalence of gendered violence and emergencies. This is because traditional norms associated with masculinities are reinforced or strengthened in times of crisis.
At these times, where family violence has previously occurred, it is likely to increase. Where family violence has not previously occurred, it is likely to commence.
Key considerations for understanding the context of family violence at times of crisis include:[157]
- the real and felt pressure experienced by men to fulfil the ‘protector and provider’ role within community, and feelings of failure and loss of control arising from a perceived failure to fulfil this role
- increased stress on people and relationships due to grief, loss, displacement, social isolation and financial instability
- within the community, unwillingness to hear about family violence and tendencies to discourage reporting and/or excuse the behaviour of perpetrators due to the stress or trauma they have experienced or because they are ‘heroes’
- community monitoring and judgement of roles performed by those within and interacting with the community
- the belief that anger is more acceptable than tears
- increased reluctance to seek help, which is commonly linked to reverting to rigid and traditional notions of masculinity, heightened sexist environments, with increased behaviours associated with hypermasculinity including erratic driving, excessive drinking and jokes
- potential increased control and isolation from the person using violence, which means it may be more difficult for services to keep risk ‘in view’
- increased unemployment and suicidality.
It is critical for anyone working in areas impacted by disaster to be aware of family violence risks for victim survivors and wellbeing and suicide risks for perpetrators.
Particular narratives or behaviours that may indicate the presence or increased risk associated with family violence include:[158]
- increased anger and quickness to anger
- increased drinking
- using behaviours that are not part of their ‘normal’ behaviours
- attempts to regain a sense of masculinity and disclosure of ’failing’ as a man
- desire to be part of a hero narrative created through perceptions of bravery.
12.1.17 Perpetrators with complex needs
People using family violence can present with and experience a multitude of complexities in their health, wellbeing and cognition. These can influence and exacerbate family violence attitudes and behaviours.
These complexities will inform your understanding, assessment and management of risk. However, they are not a reason, excuse or cause of a perpetrators’ choice to use violence.
Complex needs can include drug and alcohol use, mental illness or mental health condition, or cognitive impairment. People may have more than one complex need.
The EACPI Final report notes that not all perpetrators who present a serious risk have complex needs, and not all perpetrators with complex needs necessarily present a serious risk of family violence reoffending.
However, ‘complex needs can increase the risk of family violence (re)offending, as well as affect a perpetrator’s ability to respond to treatment for family violence offending (responsivity)’.[159]
The report also notes that ‘interventions for this cohort should address violent behaviour as well as other contributing or reinforcing factors’.[160]
You should assess and respond to people using violence using the ‘person in their context’ approach. This will support you to consider their co-occurring presenting needs and circumstances and how these impact on serious family violence risk behaviours.
Some complex needs are recognised as MARAM evidence-based risk factors, including mental illness or depression, and drug and/or alcohol misuse/abuse.
In and of themselves, these are not risk behaviours; however, they may influence the likelihood and severity of a perpetrator’s family violence behaviours.
Responding to complex needs is a key aspect of risk management.
It can support the person’s individual capacity to engage in interventions and increase the likelihood of eligibility for further interventions required to address their use of violence.
Victoria Police data cited in the EACPI Final report reveals alcohol use is involved in around 40 per cent of family violence incidents, and mental health issues as present in approximately 1 in 5 family violence incidents, with a strong association between mental illness and recidivist perpetrators.[161]
It is important to note that the reliability of this data depends on the ability of the attending police to identify it as such.
While most people with a mental illness are not violent, poor mental health and wellbeing can have a significant influence on family violence risk and suicidality. Refer to Section 12.1.15 for further information on suicide and homicide–suicide risk in the context of family violence.
Unless it is your role to diagnose a mental illness, you should not attempt to do so.
In your engagement with a person using violence, you may be able to recognise presentations of mental ill health which can inform your assessment of risk and where appropriate, may prompt you to refer the person using violence to a mental health professional.
It is important to remember that for people with mental illness who use violence, the risk presented is impacted by fluctuations in mental state.
Disturbances in mental state may be linked with likelihood, escalation, frequency and severity of violence.138
If the person is also using substances, this will further impact or cause fluctuations in mental state.
Service access and engagement barriers
The overlapping nature of these complex needs may mean it is difficult for the person to receive available treatment and support from services.
If they are referred to services that are unable address their multiple presenting needs, they may disengage and fall out of ‘view’ of the system.
In this case, carers/families can be left with the responsibility of supporting the person, which can increase risk if the person is using violence towards people who are providing care for them.
People using family violence are less likely to engage with services or follow up on referrals when they:
- present with escalating or unpredictable behaviours as a result of inconsistent or increased use of illicit drugs, alcohol, prescription drugs or inhalants
- have complex and multi-layered presentations that are difficult to discern from one another and respond to
- are moving in and out of potential psychosis
- have had traumatic experiences of institutions where violence was normalised and may have presentations of PTSD that may limit their willingness to engage with further service interventions.
Responding to perpetrators with complex needs
Professionals responding to people using violence with complex needs should be aware of appropriate referral pathways to address specific needs.
Risk management plans should include interventions that reinforce each other and are appropriately sequenced, to avoid overwhelming the person.
This can include:
- identifying any care/treatment plans that are in place and understanding the person’s engagement/compliance/adherence with the plan
- reinforcing these plans through family violence risk management plans and safety planning conversations
- exploring prior engagement with systems or services (such as justice or mental health institutions)
- considering narratives that may indicate systems manipulation or traumatic experiences that create a barrier for future engagement
- addressing these experiences/narratives when planning your risk management response
- identifying patterns or fluctuations in mental state that may be linked with escalation, frequency and severity of use of violence and may require a specific response, and any specific planning that may be required at these times.
Recognising family violence use by people with cognitive disabilities
People with cognitive disabilities have impaired cognitive functioning.
Cognitive disabilities may include acquired brain injury (ABI), neurological impairment, developmental delay, intellectual disability, mental illness or psychosocial disability and dementia, as well as cognitive impairments because of stroke or alcohol and drug use.[162]
Cognitive disabilities can affect a person’s thought processes, interpersonal skills, behaviour regulation, movement, emotions, judgement and communication. This can adversely affect the person’s independence, self-management or capacity for social, economic, cultural and educational participation.
People with cognitive disabilities may not readily present or be identified as having a disability. They might not know they have a disability, and they might not identify as having a disability.
Further, presentation and experiences can differ greatly across different types of cognitive disabilities and age groups.
For example, the developmental, life experience and necessary adjustments for a person born with an intellectual disability will differ greatly from those for a person who acquires a cognitive disability later in life.
Some cognitive disabilities may not be visible, so it is important to be aware of indicators you might observe through your engagement.
Indicators are not determinative without professional assessment, as they may indicate a range of things, including intoxication, sleep deprivation, or mental ill health.
Indicators may prompt you to ask a question or seek an assessment of cognitive disability.
These indicators of cognitive disability may include:
- distractibility and difficulty understanding concepts
- trouble with speaking and memory
- difficulty understanding or engaging with complex systems, legal information and the consequences of interventions
- unacknowledged or unrecognised delayed learning
- indications that the person is pretending to understand but does not.
If you suspect a person has a cognitive disability based on your observations or available information, you can ask some general questions about the person’s history and circumstances. This may indicate whether it is possible the person has a cognitive disability and whether they require supports or adjustments.
There is a wide range of types of cognitive disabilities, associated life experiences, and adjustments and practice considerations that may be needed.
Seek secondary consultation with disability organisations with expertise in understanding different types of disability to inform your response (refer to victim-focused Responsibility 5 and 6).
As described in Section 12.1.9, you should be guided by a social model of disability, focusing on the effects of disabling social structures, attitudes and environments and making adjustments to address these.
People with acquired brain injury who use violence
Some of the most common forms of ABI include traumatic brain injury, stroke, hypoxic brain damage, infection, tumours, and alcohol related brain damage.
ABI can result in physical, behavioural and cognitive disabilities.
People with ABI are overrepresented among both victim survivors and perpetrators of family violence.[163]
Brain Injury Australia reports that there are few studies of the prevalence of brain injury among perpetrators of family violence.
However, the evidence available indicates that rates of ABI are disproportionately high among perpetrators of family violence, compared with matched non-violent community samples and the general population.[164]
The rate of ABI among samples of male perpetrators of intimate partner violence is around 60 per cent, double the rate found in matched community samples.
Additionally, ABI is a risk factor for violent crime generally due to damage to the parts of the brain that control emotions and regulate behaviour – the behavioural outcomes of this is sometimes referred to as ‘challenging behaviours’.[165]
Due to this high prevalence, it is particularly important to ensure responses to people with ABI who use violence include necessary supports and adjustments.
ABI is characterised as damage to the brain after birth and throughout the lifespan.[166]
A person with an intellectual disability might also acquire a brain injury later in life, impacting their life in different ways.
Acquired brain injury can have a range of physical, cognitive and behavioural effects including issues with involuntary movements, balance, physical functioning and mobility, cognition (such as concentration, memory, attention), and emotional/behavioural dysregulation/impulsivity. Refer to perpetrator-focused Responsibility 3 for more detail.
Despite the strong association of challenging behaviours with ABI, the same behaviours can be equally present in those without ABI (for example, behaviours associated with poor regulation of emotions).
This highlights the importance of identifying whether there are underlying causes that contribute to the behaviours, which may inform your approach to risk assessment and management.
Service access and barriers for perpetrators
People with cognitive disabilities can experience barriers to service access and engagement, requiring alternative strategies to ensure participation on an equal basis with others.
In the context of working with people who use family violence, people with cognitive disabilities may face particular challenges when engaging with interventions such as behaviour change groups, accommodation services or in understanding information such as conditions of intervention orders.[167]
Some people with cognitive disabilities may also feel unsafe talking to police or other services, as these services might not have the training or knowledge to understand cognitive disabilities, sensitive engagement and making adjustments.
It is important to use practice techniques, such as asking the person to repeat back information in their own words. This ensures people with cognitive disability understand statements or conditions and are not just agreeing to be compliant or to ‘help’ the professional.
Having this understanding is important to inform the type and approach to interventions, and to ensure people using violence can participate, understand what is occurring and stay engaged with the service system.
As a starting point, you should always ask the person about their preferred communication method.
Adjustments might include using plain English materials, allowing the person to use any communication aids, using clear, concise language and short sentences, repeating information to confirm understanding, avoiding jargon including around medical and legal information, and providing breaks.
You may also need to conduct risk assessment conversations over time/a series of appointments, to ensure you can work with the person at their pace.
Refer to perpetrator-focused Responsibility 3 for more information on identifying cognitive disability.
Balancing practice approaches and understanding
Professionals should practice in a way that balances accountability for the use of violence with an awareness of the person’s experiences of structural inequality, which includes lack of access to resources and opportunities, ableism, ageism and disabling environments.[168]
Recognising and responding to people with cognitive disabilities who use violence requires sensitivity to the ‘lack of able-bodied privilege that these perpetrators experience in many aspects of their lives’.[169]
While experiences of marginalisation and discrimination do not excuse a person's use of violence, it is important to recognise how individuals can be both using violence and experiencing barriers of systemic ableism at the same time.
Where a person has capacity, the choice to use violence still rests with them.
The EACPI Final report outlines that complex needs, including cognitive disability, are not usually the cause of the person using violence, but require adequate identification and management to reduce the risk of the person using violence.[170]
As such, you should understand that people with cognitive disabilities can use violence while also requiring care and adjustments to increase capacity for behaviour change.
You can provide support to address both needs and behaviour concurrently.
People with cognitive disabilities may perpetrate violence towards another person with a disability or person without a disability, including intimate partners, children, carers and other family members.
You must be aware to not align with the myth that people with cognitive disabilities cannot perpetrate family violence due to their disability and are not more likely to be violent because of their cognitive disability.
People with cognitive disability need to be assessed on an individual basis without preconceptions. People with cognitive disabilities can still have capacity, and therefore responsibility, for their family violence behaviour.
The level of capacity can be conceptualised as a continuum – the severity of a person’s impairment is linked to the degree of decreased capacity.
Recognising common perpetrator presentations and narratives in relation to cognitive disability
Some common presentations that may indicate the presence of a cognitive disability or family violence behaviours[171] include:
- obsessive and controlling styles of behaviour and increased high dependence being expressed as ‘not being able to distance themselves from their partner or carer’, which relates to trying to keep partner in the relationship
- anxiety and controlling behaviours, thinking their partner will leave them due to their disability
- non-recognition of own behaviours or their impact, and to what extent they are linked to diagnosed/ undiagnosed conditions
- antisocial or risk-taking behaviours
- inability to empathise or understand the other person's perspective
- abusive behaviours that are linked to poor impulse control or reduced self-regulation
- lack of awareness or care of the consequences of actions due to inability to connect actions to reactions.
A person with a cognitive disability may use violence towards another person and minimise their responsibility by stating that the victim survivor ‘upset’ them and ‘made them use violence’.
For example, a person with ABI may avoid taking responsibility for their violence with statements like, ‘I can’t help it, I have a brain injury.’
In this case, it is important to also address their use of violence in a way that recognises their cognitive capacity and provides tailored support to them to change their behaviour.
Further guidance and approach to risk assessment and management
The perpetrator-focused MARAM Practice Guides for Responsibility 3 and 7 provide further guidance on recognising and responding to people using violence who have a cognitive disability. These focus particularly on the high prevalence of ABI and links to higher likelihood of violent crime.
Responsibility 7 provides specific guidance on strategies and adjustments in risk assessment, such as providing breaks and clear, structured questioning.
Any person using violence with suspected cognitive disability, including ABI, should be referred to a general practitioner to coordinate a referral to a rehabilitation professional for further neuropsychological or other relevant assessment (e.g., a neuropsychologist, occupational therapist, clinical psychologist).
Other referrals and supports could include linking to an occupational therapist, as well direct service and advocacy organisations that can assist with providing information on different disabilities and necessary supports and adjustments.[172]
You can seek secondary consultation for support on adjustments to service environments and interventions that meet their needs, refer to perpetrator-focused Responsibility 5.
12.1.18 Recognising high-risk perpetrators’ use of family violence
The EACPI Final report notes that some perpetrators who commit acts of family violence that cause severe physical injury or even death do not have any previous history of family violence offending.[173]
However, EACPI also cites Crime Statistics Agency data showing that most high-risk perpetrators have known histories of family violence perpetration against intimate partners.
Around 40 per cent of high-risk perpetrators are also identified as using violence against other family members and have a history of non–family violence offending.[174]
This means that many family violence perpetrators are already known to the system.
In these cases, the ongoing challenge for services is how to intervene effectively to reduce repeat violence and prevent the escalation of violence.
Recognising common high-risk perpetrator presentations
High-risk perpetrators will present to the service system with a range of co-occurring high-risk factors and behaviours. These include:[175]
- if they are younger perpetrators, displaying high risk–taking behaviours
- if they are older, having entrenched violent behaviours
- expressing strong victim stance, overwhelming sense of hopelessness and blaming of other party for their behaviour or its impacts
- holding little to no regard for legal sanctions or processes, resulting in:
- persistent breaches to legal sanctions, including intervention, corrections and family law (parenting) orders
- long criminal history, with frequent periods of imprisonment
- connections to criminal groups and gangs.
- exhibiting extreme gendered expectations and attitudes
- showing little to no capacity for empathy, present with psychopathy or sociopathy, or personality disorder
- stalking and predatory behaviours, indicated by an intense control of movement or surveillance of the victim survivor
- using sexual violence through coercion and manipulation, including attempting to ensure the victim survivor is continuously pregnant as a form of control
- having multiple victims now or over a long period of time, and/or targeting victims with actual or perceived vulnerabilities related to their needs or identity.
Some of the common presentations above are consistent with the evidence base on homicide and/or homicide–suicide in the context of family violence. Refer to Section 12.1.15 and perpetrator-focused Responsibility 3 for further information.
Service access and engagement barriers
There are very few needs-based responses available to serious risk offenders. Their contact with the service system mainly occurs through justice settings.
People operating at this level of violence often have very low voluntary engagement with services and may actively avoid contact.
Men in this cohort commonly experience feelings of system injustice and discrimination.
Responding to high-risk perpetrators with proactive and coordinated intervention
Professionals’ responsibilities to undertake active and coordinated interventions are outlined in the perpetrator-focused Responsibilities 4, 8, 9 and 10.
While opportunities for change among high-risk perpetrators are low, you should still actively manage risk through coordinated interventions.
You should identify points of potential conversation and engagement that are outside of ‘usual’ service delivery, and work collaboratively with professionals across the service system to leverage opportunities.
Any opportunity to have contact with and engage a perpetrator should be maximised. Give priority to assessing and addressing criminogenic needs.
This includes developing exit planning strategies for those leaving correctional facilities.
Perpetrators in positions of authority and impact on victim survivors
Any person in a position of power in a community or professional setting, or any role that directly relates to authority, can use that position to target their use of violence, use systems abuse or reduce access to support for victim survivors. In a community setting, these roles may include cultural, religious leaders or community social group leaders. In small metropolitan, rural or regional communities, perpetrators may be well respected and have social standing that imbues them with power, such as a school principal, local counsellor, firefighter or community sports leader.
In professional settings, perpetrators who are in significant positions of power within society, including those working in the justice system such as policing, armed and correctional services, or other recognised positions of authority or standing in the community, can present specific risks to victim survivors.
Perpetrators in these positions of authority and power may:
- have control over their family due to the nature of their employment, such as frequent redeployment, causing the victim survivor to be socially isolated and economically dependent on the person using violence[176]
- operate within a workplace culture where rigid social norms around hypermasculinity may be elevated. Workplaces where dominating and controlling behaviours are considered as leadership traits and held in high regard (i.e. military services),may diminish or discourage traits that are deemed feminine such as empathy, fear or sadness[177]
- have capacity due to their position to access information that increases risk to the victim survivor and impact on the victim survivor’s willingness to seek help(such as state-owned record management systems)
- encourage their peers to collude:
- with their narratives and behaviours to minimise or justify their use of violence[178] and/or
- limiting the service response options available to the victim survivor
- use their access to weapons to control the victim survivor.
As part of the narrative, perpetrators in positions of power may minimise, justify or shift responsibility fort heir behaviours due to the impact of their work on their health or wellbeing, or experience of trauma.They may be less likely to accept responsibility for family violence behaviours or support for related needs (such as mental illness)due to associated stigma and potential consequences such as being discharged or deemed unfit to deploy.[179]
As a result of these types of controlling behaviours and the position of authority the perpetrator is in, the victim survivor is likely to feel isolated or particularly fearful of reporting their experiences to authorities and services due to:[180]
- Fear that they will not be believed if they seek help in the community, or that as a consequence of seeking help for experiencing violence they will be ostracised from their community
- Minimisation or normalisation of the person’s use of violence due to the high level of stress they endure in their workplace. Societal acceptance that a range of occupations involving exposure to traumatic situations with often life-threatening and violent outcomes, has previously made family violence less visible and ‘normalised’ within some relationships
- Being reliant on support including housing, compensation and resources to meet basic needs (for example from ADF).Access to these may be contingent on maintaining a relationship with the person using violence, which can include accepting the role of carer to support the person using violence in their military duties, such as where the person using violence may have experiences of PTSD[181]
- Fear that the person using violence will be able to use their occupational knowledge and expertise to locate them if they leave, avoid prosecution, or manipulate the system into not believing them. People using violence in positions of power may exacerbate fears of victim survivors that system intervention cannot guarantee their safety and confidentiality
- Fear of retaliation from the perpetrator for disclosing violence where there are impacts on their employment, such as the perpetrator’s behaviour becoming known to their workplace and facing disciplinary actions or losing their job. There may be fear of increased severity of violence if the person has access and licence to use firearms
- Capacity for people in positions of power to intimidate and seek collusion from colleagues to further perpetrate, threaten or coerce a victim survivor to drop charges or withdraw family violence intervention or other orders.
Stronger positions of power and systems awareness enables perpetrators to exploit their position and standing in the method, narrative and behaviour they use to seek collusion from other professionals and services. People using violence in positions of power may have more knowledge, skill and capacity to use systems abuse behaviours to reduce victim survivors’ access to services, and navigate or weaponise systems as a method of coercive control.
People using violence in positions of power may have more knowledge, skill and capacity to use systems abuse behaviours to reduce victim survivors’ access to services.
Stronger systems awareness enables perpetrators in positions of power to understand how to seek collusion from other professionals and services with their narrative and behaviour, exploiting their position and capacity to navigate and weaponise systems as methods of coercive control.
12.2 Informing our practice
12.2.1 Perpetrator/predominant aggressor and misidentification [182]
Family violence risk assessment and management practice includes identifying:
- the person experiencing family violence (the victim survivor)
- the person using violence (the perpetrator)
- the ongoing risk of victimisation and perpetration of violence.
Correctly identifying each party is critical. This informs all immediate and ongoing strategies to reduce the risk of harm.
Harm includes the perpetrator’s use of violence and coercive control, the impact of family violence on victim survivors, and the unintentional harm or trauma created through system responses.
Identifying the person who has used a pattern of coercive, controlling and violent behaviour over time is key to identifying the perpetrator.
Where there is cross-disclosure, cross-accusations or observations of ‘mutual’ or ‘bi-directional’ violence (for further information, refer to below), the person who exhibits this pattern would be identified as the ‘predominant aggressor’ in the family relationship.
The predominant aggressor is the person causing the greatest family violence harm to a partner or family member.
Failure to identify the predominant aggressor may result in the misidentification of the victim survivor as the perpetrator.
Misidentification can lead to a number of system responses such as civil or criminal orders.
This can have long-lasting negative consequences on the victim survivor. It can lead to mistrust of police and the intervention system, resulting in reluctance to report subsequent violence.[183]
Misidentification can be due to a number of different factors. These factors include perpetrator behaviours, such as using vexatious claims or systems abuse as part of a pattern of coercive control, as well as system failures, for example, low levels of understanding about LGBTIQ relationships in parts of the service system.[184]
Perpetrators may be misidentified as victim survivors for a range of reasons.
They may use the criminal justice system to control the victim survivor by contacting the police and making false accusations.
They may also believe that they have a right to control the victim survivor by whatever means they choose, and they may express their dissatisfaction in losing control by misrepresenting themselves as a victim survivor.
Some perpetrators of family violence report being victim survivors.
A perpetrator can overtly present themselves as the victim of the violence to manipulate services, including police, and get them ‘on side’ with their narrative, resulting in the ‘real’ victim being misidentified as a perpetrator.
This tactic is a form of systems abuse and has significant impact on victim survivors.
Presenting in this way is consistent with the victim stance that many perpetrators adopt to justify and excuse their behaviour.
Perpetrators may also aim to convince service providers that they are the victim survivor or use a range of behaviours to avoid or deflect their responsibility for using family violence.
Perpetrators may also present with narratives of injustice from system interventions, which may be related to their own experiences of violence, marginalisation and discrimination.
Research evidence suggests that misidentification of victim survivors is more likely in some circumstances than others.
Those at higher risk of being misidentified include victim survivors:
- from Aboriginal communities
- from culturally, linguistically and faith-diverse communities (especially where there is a language barrier)
- with a disability
- identifying as trans and/or gender diverse
- with a mental illness
- in same-gender relationships.[185]
Some victim survivors may be misidentified as a perpetrator where they have used self-defence or violent resistance in response to their experience of the perpetrator’s pattern of violence and coercive control, or for actions taken to defend another family member.
Victim survivors are also misidentified as a perpetrator based on misinterpretation of their presentation or behaviour.
This can be due to direct and deliberate misrepresentation by the perpetrator, or due to bias on behalf of professionals and services, such as gender norms and stereotyped expectations of, for example, women’s behaviour.
Women’s behaviour is often misinterpreted in relation to:
- their response to the impact of violence on them (such as trauma responses)
- having mental health issues
- the influence of alcohol or other drugs
- perceived or actual aggression towards police or at initiation of police contact.
You should be mindful of your own biases and how these might contribute to their understandings of what a victim is ‘supposed’ to look like.
Evidence suggests notions of the ‘perfect victim’ can be highly racialised, gendered and classed, with beliefs held that a victim survivor is not supposed to fight back and be submissive to authority.[186]
There is significant evidence, however, that victim survivors are rarely passive victims of the abuse to which they are subjected.[187]
Misidentification may also occur when a perpetrator:
- falsely accuses a victim survivor of using violence or misrepresents their self-defence as evidence of violence
- cites substance misuse by the victim survivor as evidence to support their claim they are a perpetrator
- undermines a victim survivor’s presentation or behaviour as resulting from mental illness or misrepresents a victim survivor’s disability as drunkenness or being drug affected. For example, the victim survivor may be in shock or distraught as a result of the violence, they may be calm and assertive, or they may fear reprisals from showing their reaction to the violence. The perpetrator may seek to deliberately leverage commonly held discriminatory attitudes to misrepresent the victim survivor’s true state and minimise the victim survivor’s opportunity to have their voice heard.
Misidentification can also occur where a victim survivor is experiencing barriers to communication with the police or a service provider (due to trauma responses, injury or from pre-existing communication barriers).
Key indicators for identifying a predominant aggressor include:[188]
- the respective injuries of the parties
- whether either party has defensive injuries
- whether it is likely one party has acted in self-defence
- in predicting or anticipating violence, whether it is likely one party acted with violent resistance
- the likelihood or capacity of each party to inflict further injury
- self-assessment of fear and safety of each party, or, if not able to be ascertained, which party appears more fearful
- patterns of coercion, intimidation and/or violence by either party.
Other indicators include:
- prior perpetration/histories of violence (from a range of services, including specialist family violence services, health services, etc.)
- accounts from other household members or witnesses, if available
- the size, weight and strength of the parties.[189]
Where the identity of the predominant aggressor or perpetrator is unclear or not yet determined, you should record your reasoning in organisational data collecting systems so that the information can be made available to other services through information sharing.
In these situations, seek assistance from a professional with specialist skills in family violence risk assessment.
Guidance on identifying the predominant aggressor (perpetrator) is outlined in victim survivor–focused Responsibility 7 and perpetrator-focused Responsibilities 2, 3 and 7.
Challenging narratives about ‘mutual violence’ or ‘bi-directional violence’
Professionals should not use mutualising language to describe family violence, including using the terms ‘mutual violence’ and ‘bi-directional violence’ to name or describe the situation.
Mutualising language in the context of family violence can occur when:
- there are cross-accusations by parties of the other/multiple parties using violence in a family context
- professionals accept an immediate presentation of violence without further assessment and analysis of the situation
- situations are complex and the process of correctly identifying a predominant aggressor is elongated, challenging and uncertain.
Using mutualising language risks colluding with a perpetrator/predominant aggressor and undermining the safety of victim survivors.
Understanding who is causing the greatest harm can be complex in circumstances where both, or multiple, parties report they are the victim of the other.
Where there are cross-accusations, presentations or narratives that the violence is ‘mutual’ or ‘bi-directional’, take care you are not colluding with a predominant aggressor/perpetrator’s narrative to position a ‘real’ victim survivor as a perpetrator.
If a perpetrator’s victim stance is not recognised and they are provided with opportunities to collude, they may intentionally seek to manipulate professionals and services and use systems abuse to further their use of violence against the victim survivor.
Using mutualising language also risks decontextualising the experience and use of family violence from the broader situation or pattern of events.
It is important to account for the complexity and crucial distinction between violence driven by ongoing, patterned, coercive and controlling behaviours versus self-defence and violent resistance.
The perpetrator may exploit the latter through gaslighting and confusing the victim survivor, so that they view themselves as a perpetrator.
You should listen carefully to the service user’s narrative to identify situations where:
- a person reports they are using violence within a relationship, however, their disclosures indicate they experience the other person’s pattern of violence and coercive control
- a person suggests they are a victim survivor; however, their narratives indicate their use of family violence behaviours.
Presentations can be complex, and allegations of ‘mutual violence’ can occur across age groups, intimate partner and family relationships and communities, including within a family of origin context.
Responding to disclosures or cross-accusations requires specialist family violence service support.
You can seek secondary consultation and share information with specialist services for further assessment (refer to the perpetrator-focused MARAM Practice Guides – Responsibilities 2, 3, 5, 6 and 7in particular).
12.2.2 Accountability to victim survivors’ lived experience
Accountability to victim survivors is the collective responsibility of a whole service system response to family violence.
Everyone has a role to play.
A system that is accountable to victim survivors is also accountable to perpetrators, other professionals and the community more broadly.
This underpins the model of Structured Professional Judgement discussed in Section 10, which is premised on understanding the ‘expertise’ victim survivors have in the assessment of their level of safety.
It centralises victim survivors’ expertise in identifying the perpetrator’s pattern of behaviour. It builds on strategies they have already used to keep themselves safe to enhance immediate safety.
Perpetrators have an individual responsibility to be accountable for their user of violence. Specialist family violence services work with them to first acknowledge that they are using family violence before they can consider the need to stop.
Perpetrators must be personally ready to change their behaviour, and they must be stable enough in life to benefit from intervention.[190]
Perpetrators may demonstrate their readiness to change by making a personal commitment to their family’s safety and:
- acknowledging that they are using violence
- recognising their patterns of violence, rather than focusing on a few ‘signature’ examples
- developing an internal motivation to change and understanding what aspects of their behaviour and attitudes they should change
- demonstrating a capacity to change (for example, professionals can respond to needs-based issues such as homelessness and criminogenic needs that can otherwise act as significant barriers and limits to capacity for a perpetrator to change their behaviour)
- demonstrating shifts in deep-seated attitudes, starting to think differently, and applying these new attitudes in behaviour towards family members
- discarding influences that might work against these revised attitudes
- making amends for some of the damage caused
- demonstrating maintenance of any change in attitudes and behaviour achieved.[191]
Contributing to perpetrator accountability across the system
All points of the service system must take responsibility for the way in which interactions with the perpetrator can potentially make families safer, while ensuring they do not inadvertently increase risk.[192]
In aligning to the MARAM Framework, you are committing to working with a shared understanding of family violence, family violence risk, and collaborative approach to risk management.
When working with people using family violence, accountability to victim survivors’ lived experience at a systems level means:
- provide consistent information and messages that family violence is not tolerated or accepted, and that support is available
- working with others to situate the responsibility for the violence with the perpetrator
- contributing to collaborative risk management strategies that do not undermine other parts of the system response to work directly with victim survivors
- monitoring a perpetrator’s use of violence by keeping them ‘in view’
- understanding when you should seek secondary consultation or share information with specialist family violence services for comprehensive risk assessment and management, including services that work with perpetrators of violence
- reporting criminal offences or collaborating on risk management approaches before reporting
- reporting concerns about any children to Child Protection or other relevant authorities to enhance partnering with non-violent parents/adult victim survivors and increasing perpetrator accountability.
Concepts of consistent messaging, consequences and ‘in view’ are further described below.
In view
Keeping perpetrators engaged and ‘in view’ can provide current information about the level of risk presented by individual perpetrators and how this can fluctuate over time.
With this information, the service system can intervene in a timely way to identify, assess and manage dynamic and real-time risks presented by perpetrators to their family members in the short term and over time.
Perpetrators may held be ‘in view’ of the service system from many different perspectives.
Coordination and collaboration among service providers and sharing perspectives and expertise about the risk individuals present to their family members will support a comprehensive and timely ‘view’ of a perpetrator’s likelihood to use or escalate their use of violence.
Perpetrators (whether identified as such or not) will have varying motivations to engage with the service system.
These may include:
- in the normal course of using universal services, such as accessing therapeutic supports health care, education, housing or other community programs that are not related to family violence occurring within their family. These services are most likely to have more regular engagement with perpetrators, and so have an ongoing role in identification, risk assessment and management
- to seek services or justice intervention as a way of maintaining their control over the victim survivor, such as
- taking out an intervention order against the person they are perpetrating violence against
- reporting a family member to Child Protection
- destruction of property or incurring fines on behalf of the victim survivor in order to gain additional control of their resources and living requirements
- changing or making threats related to child parenting arrangements
- to seek support for themselves to address the implications of their use of family violence. These services are most likely to be accessed when needs are acute and ongoing engagement may not occur. This may include:
- reaching out to community networks such as religious or community groups
- accessing therapeutic supports such as phone counselling services to assist with parenting, mental health or housing support
- men’s sheds or specialist perpetrator’s family violence services
- to seek support for the victim of their violence. These services are most likely to be accessed when needs are acute and ongoing engagement may not occur. Seeking support for the victim survivor may be an extension of coercive and controlling behaviours. It may also be motivated by fear of the impact of their violence on the victim survivor and/or to retain the appearance of a concerned family member. This may include:
- calling emergency services
- taking a victim survivor to a hospital emergency department or health service following physical or sexual violence.
The way in which you learn of a service user’s perpetration of family violence will influence the way you engage safely with the person to:
- hold them ‘in view’
- provide consistent messages that the behaviour is unacceptable
- avoid collusion.
Consistent messaging and consequences
At a systems level, all professionals should provide consistent and reinforcing messages that violence is unacceptable in ways that are clear and respectful.
As a service system, there is a shared responsibility and aim to support and enable a perpetrator to assume personal responsibility for the use of violence and its impacts and desist from using violence.
However, the use of violence in family relationships is based on deeply held attitudes and is an intentional pattern of behaviour.[193]
Where a perpetrator comes to the attention of service providers or authorities, it is likely that they will experience external forms of accountability before (and if) they assume personal responsibility for their use of violence.
External consequences for using family violence can take a range of forms, including:
- criminal charges and sanctions
- civil remedies such as the imposition of intervention orders or family violence safety notices
- court-mandated participation in perpetrator behaviour change programs or other programs that provide case management
- a Children’s Court order for contact with their children to be supervised.
Outside the justice and statutory systems, perpetrators may feel held to account by:
- service system interventions that reinforce their accountability such as case work or opportunities to participate in culturally informed perpetrator behaviour change programs
- formal and informal community support and interventions that encourage people using violence to assume responsibility for and cease their use of violence.
What’s next and definitions
Organisations should provide information to professionals and services on the responsibilities that are applicable to their role.
What’s next?
Organisations should provide information to professionals and services on the responsibilities that are applicable to their role.
Professionals can use the appropriate chapters in the victim–survivor or perpetrator-focused MARAM Practice Guides, as appropriate to their role, to support their risk identification, assessment and management practice.
Definitions
|
Aboriginal definition of family violence |
The Victorian Indigenous Family Violence Task Force defined family violence in the context of Aboriginal communities as ‘an issue focused around a wide range of physical, emotional, sexual, social, spiritual, cultural, psychological and economic abuses that occur within families, intimate relationships, extended families, kinship networks and communities. It extends to one-on-one fighting, abuse of Indigenous community workers as well as self-harm, injury and suicide.’ The definition also acknowledges the spiritual and cultural perpetration of violence by non-Aboriginal people against Aboriginal partners which manifests as exclusion or isolation from Aboriginal culture and/or community.[194] |
|
Adolescent who uses family violence |
A young person who chooses to use coercive and controlling techniques and violence against family members, including intimate partners. Adolescents who use family violence often coexist as victims of family violence and therapeutic responses should be explored. |
|
At-risk age group |
An age group that has been identified, through evidence, as being at a higher risk of experiencing or being exposed to the negative impacts of family violence, due to their developmental stage, dependency on others or their experiencing a period of transition between dependence and independence, or vice versa. All children and young people are vulnerable to the experience of, or exposure to family violence, and some children and young people may be more vulnerable. Infants are an at-risk age group as they are more likely to be present when family violence is occurring, as compared with all other age groups, and are totally dependent on adult care to meet their needs. Risk and vulnerability diminish with increasing age of children. Adolescence, however, is also considered an at-risk age group as young people transition from dependence to independence, and if experiencing family violence in their family of origin, they are also at increased risk of experiencing violence in their intimate relationships. Older people are also recognised as an at-risk age group as at some stage they may experience ageism, and/or a period of transition from independence to dependence and become more marginalised or devalued. In addition, their social and community connections can diminish over time and these factors can result in increased vulnerability to mistreatment and abuse. |
|
Characteristics of person using violence linked to serious risk |
Key behaviours and traits of a person using violence that indicate they are more likely to present a serious risk, including greater likelihood of escalated and severe family violence risk, can include levels of jealousy and hostility, violence directed towards general community as well as family members, pro-violence attitudes, limited capacity for empathy and remorse and low receptivity to system interventions. They generally have very low voluntary engagement with services and may actively avoid contact. Characteristics of the person posing serious risk of family violence, considered alongside the assessed pattern and history of coercive control, complex needs and circumstances, will inform the determination of level of risk and active and coordinated risk management intervention strategies. |
|
Child |
Has the meaning set out in section 4 of the FVPA, being a person who is under the age of 18 years (which includes infants and adolescents). |
|
Cisgender |
People whose gender identity is in line with the social expectations of their sex assigned at birth, that is, those who are not transgender. |
|
Coercive control |
Coercive control can be exerted through any combination of the evidence-based family violence risk factors. It is often demonstrated through patterned behaviours of emotional, financial abuse and isolation, stalking (including monitoring of technology), controlling behaviours, choking/strangulation, sexual and physical violence. The behaviour is intended to harm, punish, frighten, dominate, isolate, degrade, monitor or stalk, regulate and subordinate the victim survivor. One occurrence of family violence behaviour can create the dynamic of ongoing control, due to the threat of possible future family violence and the resultant ongoing fear, even if ‘high-risk’ behaviours do not re-occur. People using violence exert coercive control using a range of behaviours over time, and their effect is cumulative. Everyone experiencing family violence is experiencing coercive control. |
|
Collusion |
Refers to ways that an individual, agency or system might reinforce, excuse, minimise or deny a perpetrator’s violence towards family members and/or the extent or impact of that violence. Collusion can take many forms (verbal and non-verbal), it can be conscious or unconscious and it includes any action that has the effect of reinforcing the perpetrator’s violence-supportive narratives as well as their narratives about systems and services. |
|
Commonwealth Privacy Act |
Privacy Act 1988 (Cth) |
|
Culturally safe responses |
To practice in a culturally safe way means to carry out practice in collaboration with the service user, with care and insight for their culture, while being mindful of one’s own. A culturally safe environment is one where people feel safe and where there is no challenge or need for the denial of their identity. |
|
CYFA |
Children, Youth and Families Act 2005 (Vic) |
|
Diverse communities |
Diverse communities include the following groups: diverse cultural, linguistic and faith communities; people with a disability; people experiencing mental health issues; lesbian, gay, bisexual, transgender and gender diverse, intersex and queer/questioning (LGBTIQ) people; women in or exiting prison or forensic institutions; people who work in the sex industry; people living in regional, remote and rural communities; male victims; older people and young people (12 to 25 years of age). |
|
Elder |
An older person, as defined below. In Aboriginal communities, Aboriginal Elders hold valued positions and are recognised for their strong leadership, wisdom, expertise and the contributions they make to the Aboriginal community. |
|
Elder abuse |
Is any harm or mistreatment of an older person that is committed by someone with whom the older person has a relationship of trust. In the context of family violence, this may be elder abuse by any person who is a family member (such as their partner or adult children) or carer. Elder abuse may take any of the forms defined under ‘family violence’. |
|
Family violence |
Has the meaning set out in section 5 of the FVPA which is summarised here as any behaviour that occurs in family, domestic or intimate relationships that is physically or sexually abusive; emotionally or psychologically abusive; economically abusive; threatening or coercive; or is in any other way controlling that causes a person to live in fear for their safety or wellbeing or that of another person. In relation to children, family violence is also defined as behaviour by any person that causes a child to hear or witness or otherwise be exposed to the effects of the above behaviour. This definition includes violence within a broader family context, such as extended families, kinship networks and communities. |
|
Family violence assessment purpose |
Has the meaning set out in section 144A of the FVPA, being the purpose of establishing or assessing the risk of a person committing family violence or a person being subjected to family violence. |
|
Family violence protection purpose |
As defined in the FVPA to mean the purpose of managing a risk of a person committing family violence (including the ongoing assessment of the risk of the person committing family violence) or a person being subjected to family violence (including the ongoing assessment of the risk of the person being subjected to family violence). |
|
FOI Act |
Freedom of Information Act 1982. |
|
Framework |
The Family Violence Risk Assessment and Risk Management Framework approved by the relevant Minister under section 189 of the FVPA. |
|
Framework organisation |
An organisation prescribed by regulation to be a framework organisation for the purposes of Part 11 of the FVPA and required to align their policies, procedures, practice guidance and tools to it. References in this document to framework organisations include section 191 agencies. |
|
FVPA |
Family Violence Protection Act 2008. |
|
Guidelines |
The Family Violence Information Sharing Guidelines issued by a Minister under section 144P of the FVPA. |
|
Imminence of risk |
Likelihood of risk of harm or death escalating immediately or within a short timeframe. |
|
In view |
To keep the person using violence visible to the service system. Actively monitoring changes to risk behaviours used and the coordination and collaboration of service providers to intervene in a timely way to reduce or remove risk and support safety. Keeping perpetrator’s risk in view holds them to account for their use of family violence and supports them to change their behaviour. |
|
Intent |
The purpose or aim for the person’s choice to use family violence. Intent is a significant predictor of whether a behaviour will occur. Understanding a person’s intent and end objective of their use of violence helps professionals to establish a picture of dynamic risk factors associated with beliefs and attitudes. Intent should be understood in the context of coercive control. |
|
Intersectionality |
Refers to the structural inequality and discrimination experienced by different individuals and communities, and the impact of these creating barriers to service access and further marginalisation. Intersectionality is the complex, cumulative way in which the effects of multiple forms of identity-based structural inequality and discrimination (such as racism, sexism, ableism and classism) combine, overlap or intersect, in the experiences of individuals or communities.[195] These aspects of identity can include gender, ethnicity and cultural background, language, socioeconomic status, disability, sexual orientation, gender identity, religion, age, geographic location or visa status. |
|
ISE |
Information sharing entity as defined in the FVPA to be a person or body prescribed, or a class of person or body prescribed, to be an information sharing entity. |
|
LGBTIQ |
Lesbian, gay, bisexual, transgender and gender diverse, intersex and queer/questioning. |
|
MARAM Framework |
The Family Violence Multi Agency Risk Assessment and Management Framework. |
|
Misidentification |
Where a victim survivor of family violence is named or categorised as a perpetrator (or respondent in criminal proceedings) for their use of self-defence or violent resistance, or as a form of defence of another family member, or where they are identified based on a misinterpretation of their presentation due to the impact of violence, mental health issues, influence of alcohol or other drugs, aggression towards policy or initiation of police contact. |
|
Needs |
Refer to protective and stabilisation factors below. |
|
Older people |
Any person who is aged 65 or older, any Aboriginal Victorian aged 45 or older. |
|
Perpetrator |
Has the same meaning as the words ‘a person of concern’ in section 144B of the FVPA. The FVPA provides an individual is a person of concern if an information sharing entity reasonably believes that there is a risk that they may commit family violence. This will have been identified by undertaking a framework-based family violence risk assessment. |
|
Perpetrator accountability |
The process by which the perpetrator themselves acknowledges and takes responsibility for their choices to use family violence and work to change their behaviour. It sits with all professionals, organisations and systems through their collective, consistent response to promote perpetrators’ capacity to take responsibility for their actions and impacts, through formal or informal services response mechanisms. |
|
Person in their context |
This term refers to the practice of taking a holistic and comprehensive view of the perpetrator. It supports practitioners to form an understanding of the perpetrator’s history, experiences, circumstances, presenting needs, current environment and relationships in order to determine and assess aspects of their life that are contributing to their choice to use family violence risk behaviours. This includes developing an understanding of the person’s behaviours in context to their expressed values, beliefs, attitudes, and personality characteristics. |
|
Predominant aggressor |
The term predominant aggressor seeks to assist in identifying the actual perpetrator in the relationship, by distinguishing their history and pattern of coercion, power and controlling behaviour, from a victim survivor who may have used force for the purpose of self-defence or violent resistance in an incident or series of incidents. The predominant aggressor is the perpetrator who is using violence and coercive control to dominate, intimidate or cause fear in their partner or family member, and for whom, once they have been violent, particularly use of physical or sexual violence, all of their other actions take on the threat of violence. |
|
Protection entity |
A prescribed information sharing entity that is authorised to request information for a family violence protection purpose. |
|
Protective and stabilisation factors |
Factors identified that, when strengthened, promote safety, stabilisation and recovery from family violence, such as intervention orders, housing stability and safety, health responses, support networks, financial resources and responding to wellbeing and needs. Protective factors are often referred to when professionals undertake needs assessment. When engaging with a person using violence, identifying and responding to these factors enables professionals to understand a ‘person in their context’. This lens supports targeted and tailored risk management responses to their use of violence. Where protective factors are strengthened, it may reduce the likelihood of continued use of some forms of family violence and increase capacity for behaviour change. Consideration of protective and stabilisation factors provides an understanding of contextual factors related to their use of violence, not a justification for it. |
|
Queer |
Queer is an umbrella term used by some people to describe non-conforming gender identities and sexual orientations. Queer includes people who are questioning their gender identity and sexual orientation. |
|
Reasonable belief threshold |
A reasonable belief requires the existence of facts that are sufficient to induce the belief in a reasonable person. Belief requires something more than suspicion.[196] |
|
Regulations |
The Family Violence Protection (Information Sharing and Risk Management) Regulations 2018. |
|
Risk assessment |
The process of applying the model of Structured Professional Judgement to determine the level of family violence risk. |
|
Risk assessment entity |
Has the same meaning as set out in the FVPA, being an information sharing entity that is prescribed to belong to the category of a risk assessment entity. Risk assessment entities can request and voluntarily receive information from ISEs for a family violence assessment purpose. |
|
Risk identification |
Recognising through observation or enquiry that family violence risk factors are present, and then taking appropriate actions to refer or manage the risk. |
|
Risk factors |
Evidence-based factors that are associated with the likelihood of family violence occurring or the severity of the risk of family violence. |
|
Risk management |
Any action or intervention taken to reduce the level of risk presented to a victim and hold perpetrators to account. Actions taken and interventions that are implemented appropriate to the level of risk identified in the risk assessment stage. Risk management includes supports or interventions that promote stabilisation and recovery from family violence for victim survivors. Risk management includes responding to circumstances and presenting needs of perpetrators that reduce likelihood of use of related risk behaviours. |
|
Routine screening |
The use of family violence specific screening questions, asked of all individuals engaged with a service in the intake/screening/initial consultation phase. |
|
Safety planning |
Safety planning involves a conversation by a professional who is working with an adult or child victim survivor, or a person using violence, about actions they can take to respond to family violence risk of the person using violence. When working with a victim survivor, a safety plan documents strategies to help manage their own safety in the short to medium term; building on what the victim survivor is already doing and what works for their circumstances, to resist control, manage the impacts of the perpetrator’s behaviour and other actions aimed at keeping themselves safe. When working with a perpetrator, safety plan assists them to take responsibility for recognising their needs and circumstances that relate to escalating family violence risk behaviours; stopping their use of risk behaviours against family members, including through de-escalation strategies; self-initiating engagement with professional services when their circumstances change or use of risk behaviours escalates (risk to victim survivors or risk to self (suicide or self-harm)). |
|
Screening |
The use of questions to explore the possibility of family violence being present, due to concerns through observation or other assessment. |
|
Section 191 agency |
Has the same meaning as section 188 of the FVPA, being an agency that a public service body or public entity enters into or renews a state contract or other contract or agreement in accordance with section 191 and that provides services under that contract or agreement that are relevant to family violence risk assessment or family violence risk management. References in this document to Framework organisations include section 191 agencies. |
|
Serious risk |
Risk factors associated with the increased likelihood of the victim survivor being killed or nearly killed. |
|
Service |
Provision of a specific support or providing a formalised level of assistance, which is of benefit to individuals in the community. |
|
Service provider |
Businesses, organisations, or other professional groups which provide a service or range of services, to the benefit of individuals in the community. |
|
Seriousness of risk |
The level of risk assessed to be present, indicating the likelihood that the victim/s will be seriously harmed, killed, or be subjected to an escalation of the family violence perpetrated against them. |
|
Systems abuse |
People who use family violence may seek to manipulate actions or decisions of professionals in the system as a method to further coerce and control victim survivors. This can come in the form of vexatious applications to courts (which are particularly prevalent in family law proceedings) or malicious reports to statutory bodies such as police, health services, family services and Child Protection. People using violence may target the identity of a victim survivor to leverage structural inequality or barriers they experience as a form of systems abuse. Systems abuse can also lead to misidentification of people using family violence and victim survivor. Systems abuse should be considered in the context of broader understandings of coercive control – it is a strategy to maintain control over a victim survivor or cause further harm. |
|
The Royal Commission |
The Victorian Royal Commission into Family Violence. |
|
Third party |
Has the same meaning as the words ‘a linked person’ in section 144A of the FVPA, being any person whose confidential information is relevant to a family violence assessment purpose or family violence protection purpose other than a person who is a primary person (i.e., the victim survivor), a person of concern (i.e., the perpetrator) or is alleged to present a risk of family violence (i.e., alleged perpetrator). |
|
Transgender |
People whose gender identity differs from the social expectations of their sex assigned at birth. That is, a person who is not cisgender. |
|
Victim stance |
A person using violence may present a victim stance to reduce taking responsibility for their own behaviours, or deflect from admitting the harm they have caused. It often presents through minimising, denying, justifying or blame-shifting narratives. A person using violence may also highlight their past experiences of violence, trauma, or systems barriers when discussing the violence. This tactic invites professionals to collude with the person using violence and adopt beliefs about who is responsible or less responsible for the violence. This can result in misidentification of the person using violence and victim survivor. Presenting a victim stance enables a person using violence to minimise responsibility-taking by placing blame on their experiences as the ‘cause’ of their use of violence. It can be a tactic to deflect professionals' attention to factors outside the person using violence's control and cover up the choices they have made or continue to make. |
|
Victim survivor |
Has the same meaning as the words ‘a primary person’ (adult or child) in the FVPA. The FVPA provides a person is a primary person if an information sharing entity reasonably believes there is risk that the person may be subjected to family violence. |
|
Women who use force |
Is used to describe victim survivors who, in their intimate partner relationships, have used force in response to violence from a predominant aggressor/perpetrator. This can be identified through recognising the history and pattern of ongoing perpetration of violence against them. |
Footnotes
Footnotes from the MARAM practice guides: Foundation knowledge guide.
[1] Kertesz M et al. 2019, Women who use force: final report – vol.1, University of Melbourne, Melbourne, p. 4.
[2] This description is based on self-report and is in no way representative of any value judgement related to actual strength/weakness of a victim survivor, refer to Kertesz M et al. 2019, Women who use force: final report – vol. 1, University of Melbourne, Melbourne, p. 21.
[3] Adapted from EACPI 2019, Final report, which cites Smith, Humphreys and Laming 2013, ‘The central place of women’s support and partner contact in men’s behaviour change programs’, Ending Men’s Violence Against Women and Children, vol. 1, no. Spring 2013, p. 293.
[4] This includes a strong focus on information sharing and coordinated, collaborative practice between services.
[5] State of Victoria 2016, Royal Commission into Family Violence: Summary and recommendations, Parl Paper No 132 (2014–16), Summary and recommendations, p. 7.
[6] Ibid., p. 1.
[7] Note, some descriptions of expectations have been amended or corrected. This is due to change in definition or title of assessment or management tools, approaches. Further information on expectations for each responsibility is provided in the ‘Learning objectives’ section of each practice guide.
[8] Includes victim survivor specialist services and perpetrator intervention services, such as men’s behaviour change and case management specialist services.
[9] Legal services are currently not prescribed as framework organisations, but still have a role in identifying, assessing and managing risk.
[10] The Royal Commission and the Expert Advisory Committee on Perpetrator Interventions identified key opportunity workforces to respond to intersections of behaviours linked to aperpetrator’scircumstances, including mental health, alcohol and other drugs, housing/homelessness, community isolation, unemployment, connection with Child Protection, Victoria Police, courts and correction services.
[11] Victorian Indigenous Family Violence Taskforce 2003, definition used in Department of Health and Human Services 2018, Dhelk Dja: Safe Our Way – Strong Culture, Strong Peoples, Strong Families, State Government of Victoria, Melbourne.
[12] Family Violence Protection Act 2008 (Vic), s. 5.
[13] Victim survivors who use force in response to a predominant aggressor/perpetrator are not identified as perpetrators for the purpose of assessing coercive control. Guidance on assessing predominant aggressor is included in the MARAM Practice Guides.
[14] Stalking and monitoring behaviour includes technology-facilitated abuse that enables the perpetrator’s surveillance of the victim survivor and can be the method for delivery of threatening behaviour.
[15] Stark E 2009, ‘Rethinking coercive control’, Violence against Women, vol. 15, no. 12, pp. 1509–25; Westmarland N and Kelly L 2013, ‘Why extending measurements of “success” in domestic violence perpetrator programmes matters for social work’, British Journal of Social Work, vol. 43, no. 6, pp. 1092-1110.
[16] Scope defined in reference to Stark E 2020, ‘The “Coercive Control Framework”: What makes law work for women?’, Criminalising Coercive Control, pp. 33–49.
[18] There may be family violence occurring in more than one intimate partner relationship, such as if there are non-monogamy or multiple partner relationships.
[19] Department of Health and Human Services 2018, Dhelk Dja: Safe Our Way – Strong Culture, Strong Peoples, Strong Families, State Government of Victoria, Melbourne.
[20] Definition of family violence in Ibid., p. 7. Professionals should read and be guided by the full definition of family violence and principles outlined in Dhelk Dja to complement practice approaches for working with Aboriginal communities under the MARAM Framework and Practice Guides.
[21] Note, ’breach’ is used throughout these guides as it is the term used across the broader service system. Some statutory settings may use the term ’contravention’ which has the same meaning.
[22] Women comprised 73 per cent of all intimate partner homicides in Australia during the 2018–19 reporting period; Bricknell S and Doherty L2021, Homicide in Australia 2018–19, statistical report no. 34, Australian Institute of Criminology, Canberra.
[23] Australian Domestic and Family Violence Death Review Network 2018, Australian Domestic and Family Violence Death Review Network: 2018 data report, ADFVDRN, Sydney, p. xii.
[24] Ibid., p. xii.
[25] State of Victoria 2016, Royal Commission into Family Violence: Report and recommendations, Vol II, Parl Paper No 132 (2014–16), p. 103.
[26] Crime Statistics Agency, ‘Family Violence Data Portal – Victoria Police, Youth involved family incidents’, www.crimestatistics.vic.gov.au/family-violence-data-portal/family-violence-data-dashboard/victoria-police, accessed May 2021. This data relates to police-attended incidents only. It does not capture family violence experienced by children that is police attended.
[27] Ibid.
[28] Ibid.
[29] Biphobia, homophobia and transphobia are the outcome of cisnormativity and heteronormativity.
[30] Evidence-based risk factors developed in international jurisdictions, and in Australia, are largely derived from reviews of coronial inquests into family violence homicides.
[31] This can occur where family violence by a perpetrator causes the emotional or physical absence of other adult or child family members who would normally care for that child.
[32] These examples of sexualised behaviour toward children are crimes.
[33] This refers to behaviours where this is used as a tactic of a perpetrator for power and control, not actions of a parent/carer to keep their child/children safe from a perpetrator.
[34] This is where family violence is established as present through risk assessment. In some instances, engagement with, for example, child protection, has been instigated as a controlling behaviour by one party over another.
[35] Authorisation to share adult victim survivor information under the Family Violence Information Sharing Scheme requires consent, unless there is serious risk, or the information is relevant to assessing child risk.
[36] Adapted from Crenshaw K 1989, ‘Demarginalizing the intersection of race and sex: a black feminist critique of antidiscrimination doctrine, feminist theory and antiracist politics’, The University of Chicago Legal Forum, vol. 1989, pp. 139-167. In its original discourse, intersectional analysis focused on race and sex.
[37] State of Victoria 2019, Everybody matters: inclusion and equity statement, State of Victoria, Melbourne.
[38] Adapted from OurWatch 2019, Men in focus, pp. 34-35.
[39] Definition and section informed by Klinic Community Health 2013, Trauma-informed: the trauma toolkit, 2nd ed.; and Kezelman C and Stavropoulos 2018, Talking about trauma: guide to conversations and screening for health and other service providers, Blue Knot Foundation, p. 10.
[40] Adapted from Kezelman C and Stavropoulos 2012, ‘The last frontier – practice guidelines for the treatment of complex trauma and trauma-informed care and service delivery’, Adults Surviving Child Abuse, p. 53.
[41] State of Victoria 2021, Royal Commission into Victoria’s Mental Health System final report: vol. 2 – collaboration to support good mental health and wellbeing, Parl. Paper no. 202, p. 347.
[42] Ibid., p. 348.
[43] Ibid., p. 349.
[44] Varcoe CM, Wathen CN, Ford-Gilboe M, Smye V and Browne 2016, VEGA briefing note on trauma- and violence-informed care, VEGA Project and PreVail Research Network, Ottawa, p. 1.
[45] Ibid.
[46] Kezelman C and Stavropoulos P2012, The last frontier: practice guidelines for treatment of complex trauma and trauma informed care and service delivery, Adults Surviving Child Abuse (now Blue Knot Foundation), p. 49.
[47] Substance Abuse and Mental Health Services Administration (SAMHSA) 2014, Concept of trauma and guidance for a trauma-informed approach, U.S. Department of Health and Human Services, Rockville, p. 9.
[48] Kezelman C and Stavropoulos P2012, op. cit., p.79.
[49] Department of Health and Human Services (USA) 2014, SAMSHA’s concept of trauma and guidance for a trauma-informed approach, p.8.
[50] Ibid.
[51] Department of Health and Human Services 2018, Dhelk Dja: Safe Our Way – Strong Culture, Strong Peoples, Strong Families, State Government of Victoria, Melbourne, p. 29.
[52] Family Safety Victoria 2019, The Nargneit Birrang Framework: Aboriginal Holistic Healing Framework for Family Violence, p.21
[53] Ibid.
[54] ANROWS 2015,Promoting community-led responses to violence against immigrant and refugee women in metropolitan and regional Australia: the ASPIRE Project – state of knowledge paper, ANROWS, p. 21.
[55] Ibid.
[56] Not all perpetrators have a history of trauma. However, applying a practice model will enable professionals to identify whether this is present and to work safely where it is.
[57] No to Violence 2020, NSW risk, safety and support framework, No to Violence, Melbourne.
[58] ANROWS 2017, Summary of findings from the 2017 National Community Attitudes towards Violence Against Women Survey, ANROWS, p. 2.
[59] It is common for there to be cross-allegations of violence from each person in LGBTIQ intimate partner relationships. This may give the impression there is ‘mutual violence’ occurring. Specialist family violence services (including specialist LGBTIQ services) can support ongoing assessment to identify if there is a predominant aggressor/perpetrator who is not easily identifiable in the first instance. Refer to Section 12.2.1 of this Foundation Knowledge Guide and Responsibility 6 for more information.
[60] Our WATch 2015 Change the Story, p. 8.
[61] This section discusses cisgendered men and masculinity. Information on masculinity and performativity in other communities is discussed further in later sections of this guide.
[62] Adapted from OurWatch 2019, Men in focus, p. 36.
[63] Ibid.
[64] Ibid., p. 37.
[65] Ibid., p. 36, quoting Murdolo and Quiazon 2016, Key issues in working with men from immigrant and refugee communities in prevention violence against women, White Ribbon Australia Research Series.
[66] Ibid.
[67] Ibid. p. 45. These are consistent with social pressures identified in the Man Box attitudes to manhood and behaviours of young men in Australia, and internationally, as outlined in The Men’s Project and Flood M 2018, The Man Box: a study on being a young man in Australia. Jesuit Social Services, Melbourne.
[68] ANROWS 2017 notes that while there has been general attitudinal improvement from 2009–2017, there are still gender differences, with men having a lower understanding of violence against women, a lower level of support for gender equality and a higher level of attitudinal support for violence against women.
[69] This may include a perpetrator’s use of technology-facilitated abuse resulting in the victim survivor having reduced access to social media or technology due to fear of monitoring or surveillance.
[70] Hill AO, Bourne A, McNair R, Carman M and Lyons A 2020, Private Lives 3: the health and wellbeing of LGBTIQ people in Australia, monograph series no. 122, ARCSHS, Melbourne.
[71] Crime Statistics Agency 2020, Family violence data dashboard, accessed October 2020. This outlines that most male victims experience violence from other male family members (as children from parents, siblings, other family members). However, for most men killed in family violence incidents, the respondent was a current or former intimate partner where the male victim was identified as a predominant perpetrator of violence; Australian Institute of Health and Welfare 2019, Family, domestic and sexual violence in Australia: continuing the national story, AIHW, Canberra, p. 49–53 <https://www.aihw.gov.au/getmedia/b0037b2d-a651-4abf-9f7b-00a85e3de528/a…;, accessed October 2020. This outlines that most family violence homicide victims were female (59 per cent), almost 2 in 3 (64 per cent) were female victims and 1 in 4 (75 per cent) male victims were killed by an intimate partner. More than 3 in 4 (75 per cent) of all perpetrators of family violence homicide were male.
[72] AIHW 2018, Family, domestic and sexual violence in Australia, p xi, notes that ‘In 2011, it contributed to more burden of disease (the impact of illness, disability and premature death) than any other risk factor for women aged 25–44.’
[73] Information in this section is summarised from the MARAM Framework.
[74] Australian Institute of Criminology 2017, Homicide in Australia: 2012–2013 to 2013–2014: National Homicide Monitoring Program.
[75] Australian Institute of Health and Welfare, Family, domestic and sexual violence in Australia, 2018, page ix.
[76] Parliament of Australia 2014, Domestic, family and sexual violence in Australia: an overview of the issues.
[77] For example, Stark E 2007, Coercive control: how men entrap women in personal life, Oxford University Press, Oxford.
[78] DVRCV and WLSV 2013, Serious invasions of privacy in the digital era: submission to the Australian Law Reform Commission Review.
[79] This section refers to cis-gendered men and women. Experiences of use of violence against trans and non-binary people are covered in Section 12.1.7 and 12.1.8.
[80] Seidler K 2010, Crime, culture and violence: understanding how masculinity and identity shapes offending, 1st ed., Australian Academic Press, Bowen Hills.
[81] ANROWS 2012, Violence against women: additional analysis of the Australian Bureau of Statistics’ Personal Safety Survey,ANROWS, Sydney, p. 30.
[82] Ibid, p 4.
[83] Ibid.
[84] Judd F, Armstrong S and Kulkarni J 2009, ‘Gender-sensitive mental health care’, Australasian Psychiatry, vol. 17, no. 2, pp. 105-111. doi:10.1080/10398560802596108
[85] ABS 2017, Causes of Death, ABS, Canberra
[86] American Psychological Association 2018, APA guidelines for psychological practice with boys and men,APA, Washington DC.
[87] Levant RF and Wimer DJ 2013, ‘Masculinity constructs as protective buffers and risk factors for men’s health’. American Journal of Men's Health, vol. 8, no. 2, pp. 110-120.
[88] Richards M and Bedi RP 2015, ‘Gaining perspective: How men describe incidents damaging the therapeutic alliance’, Psychology of Men & Masculinity, vol. 16, no. 2, pp. 170-182.
[89] Hegarty K, Tarzia L, Forsdike K, Vlais R, Flood M, Feder G and Humphreys C 2016, Final report: promoting early intervention with men's use of violence in relationships through primary care (PEARL study), APHCRI, Canberra.
[90] Adapted from Central and Eastern Sydney Primary Health Network 2019, The impact of domestic violence on mother child relationships. This section uses gendered language in recognition of prevalence, but perpetrators’ behaviour targeted to undermine a parent–child relationship against a non-violent parent/carer can occur within any family relationship.
[93] McGinn T, McColgan M, Taylor B 2020, ‘Male IPV perpetrator’s perspectives on intervention and change: a systematic synthesis of qualitative studies’, Trauma, Violence, & Abuse, vol. 21, no. 1, pp. 97-112.
[94] Australian Institute of Family Studies 2015, Children’s exposure to domestic and family violence: Key issues and responses, CFCA Paper No. 36.
[95] The Family Law Act 1975 focuses on the rights of children and the responsibilities that each parent has towards their children, rather than on parental rights. The Act aims to ensure that children can enjoy a meaningful relationship with each of their parents and are protected from harm.
[96] Humphreys C and Campo M 2017, Fathers who use violence: options for safe practice where there is ongoing contact with children, CFCA paper no. 43, AIFS, Canberra.
[97] Such as any child who identifies as LGBTIQ, particularly trans or non-binary children, or children who are Aboriginal or from a diverse community that one or both parents do not also identify with.
[98] State of Victoria 2016, Royal Commission into Family Violence: Report and recommendations, Vol II, Parl Paper No 132 (2014–16) Chapter 10, Perpetrators, p. 270.
[99] Ibid., Chapter 10, Responses to children and young people experiencing family violence, p. 123.
[100] Perel G and Peled E 2008, ‘The fathering of violent men: constriction and yearning’, Violence Against Women, vol. 14, no. 4, pp. 457-482.
[101] Department of Health and Human Services 2018, Dhelk Dja: Safe Our Way – Strong Culture, Strong Peoples, Strong Families, State Government of Victoria, Melbourne.
[102] Australian Institute of Health and Welfare 2018, Domestic and sexual violence in Australia, AIHW, Canberra, p. ix.
[103] Department of Health and Human Services 2018, Dhelk Dja: Safe Our Way – Strong Culture, Strong Peoples, Strong Families, State Government of Victoria, Melbourne; Braybrook A 2015, ‘Family violence in Aboriginal communities’, DVRCV Advocate, www.dvrcv.org.au/sites/default/files/Family-violence-in-Aboriginal-communities-FVPLS.pdf, accessed 12 October 2019.
[104] Elder abuse that is not within the definition of family violence may also include social abuse or neglect, abuse by trusted others, or abuse that is experienced in service or institutional settings, such as professional misconduct by paid carers. These forms may relate to behaviour that is centred around ignorance or negligence, such as carer stress.
[105] This may depend on the circumstances of the financial abuse.
[106] For example, neglect that results in physical assault or harm.
[107] Bagshaw D et al. 2013, ‘Financial abuse of older people by family members: views and experiences of older Australians and their family members’, Australian Social Work, vol. 66, no. 1, pp. 123-133; Association for Conflict Resolution 2015, ‘Elder mediation and the financial abuse of older people by a family member’, Conflict Resolution Quarterly.
[108] The Royal Commission noted instances where victim survivors of sexual abuse by older men with dementia were not recognised by health professionals as being abused. Norma’s Project also found there is evidence to suggest that sexual abuse against older women is likely to be underreported. Mann R, Horsley P, Barrett C, Tinney J 2014, Norma’s Project. a research study into the sexual assault of older women in Australia, ARCSHS monograph series no. 98, ARCHSH, Melbourne.
[109] Medical Treatment Planning and Decisions Act 2016 (Vic), ss 4, 7; Guardianship and Administration Act 2019 (Vic), ss 5, 8, 9.
[110] Service providers have obligations to provide reasonable adjustments for people with disabilities under the Equal Opportunity Act 2010 (Vic).
[111] This is commonly identified in health service settings.
[112] Australian Institute of Family Studies 2015, Intimate partner violence in lesbian, gay, bisexual, trans, intersex and queer communities, CFCA professional resource, AIFS, Canberra, pp 3-4.
[113] Hill AO, Bourne A, McNair R, Carman M and Lyons A 2020, Private Lives 3: the health and wellbeing of LGBTIQ people in Australia. ARCSHS monograph series no. 122, ARCSHS, Melbourne.
[114] OurWatch 2017, Primary prevention of family violence against people from LGBTI communities: an analysis of existing research, p. 49.
[115] Hill AO, Bourne A, McNair R, Carman M and Lyons A 2020, op. cit., pp. 70-74.
[116] Hill AO, Lyons A, Jones J, McGowan I, Carman M, Parsons M, Power J, Bourne A 2021, Writing Themselves In 4: the health and wellbeing of LGBTQA+ young people in Australia, national report, monograph series no. 124, ARCSHS, Melbourne, p. 10.LGBTIQ young people (aged 16 to 17 years) were five times more likely to seriously consider attempting suicide in the past 12 months than the general population. And 1 in 10 aged 16 to 17 had attempted suicide in the past 12 months, almost three times the general population. In addition, one in four 16–17-year-old LGBTIQ young people had attempted suicide in their lifetimes, four times the rate of the general population.
[117] State of Victoria 2017, Absolutely everyone: state disability plan 2017–2020, p. 9.
[118] ANROWS 2016, A preventable burden: Measuring and addressing the prevalence and health impacts of intimate partner violence in Australian women, Compass 7, p. 3.
[119] Women with Disabilities Victoria 2014, Position statement: Violence against women with disabilities.
[120] Women with Disabilities Australia 2013, Stop the violence: Addressing violence against women and girls with disabilities in Australia, background paper, p. 27.
[121] Women with Disabilities Victoria 2014, op. cit.
[122] Service providers have obligations to provide reasonable adjustments for people with disabilities under the Equal Opportunity Act 2010 (Vic).
[123] Victoria Legal Aid 2020, Achieving safe and certain homes for children: Recommendations to improve the permanency amendments to the Children, Youth and Families Act 2005 based on the experience of our clients. This report states that since the introduction of the permanency amendments to the Children, Youth and Families (Permanent Care and Other Matters) Act 2014, 19 per cent of children who had a parent with a disclosed disability were removed from their parents and are not on a reunification pathway, compared with 11 per cent of children whose parents did not have a disclosed disability (p. 14); Carter B 2015, Rebuilding the village: supporting families where a parent has a disability, Report No 2, Office of the Public Advocate, p. 4.
[124] Wehmeyer ML, Shogren K, Angel Verdugo M, Nota L, Soresi S, Lee S-H and Lachapelle Y 2014, ‘Cognitive impairment and intellectual disability’, Special education international perspectives: biopsychosocial, cultural, and disability aspects, Emerald Group, pp. 55-89.
[125] You can find more information at the Office of the Public Advocate’s phone advice line and website about the role of guardians and working with people under guardianship. This includes considering the role of supported decision-making to guide people with cognitive disabilities to exercise their rights and make decisions, including through risk management and safety planning.
[126] Ibid.
[127] Brain Injury Australia 2018, The prevalence of acquired brain injury among victims and perpetrators of family violence.
[128] Jamieson LM, Harrison JE and Berry JG 2008, ‘Hospitalisation for head injury due to assault among Indigenous and non-Indigenous Australians, July 1999 – June 2005’, Medical Journal of Australia, vol. 188, no. 10.
[129] Read J, Harper D, Tucker I and Kennedy A 2018. ‘Do adult mental health services identify child abuse and neglect? A systematic review’, International Journal of Mental Health Nursing, vol. 27, pp. 7-19.
[130] Australian Institute of Criminology 2004, Women’s experience of male violence, findings from the Australian component of the International Violence Against women survey.
[131] Khalihef H, Moran P, Borschmann R, Dean K, Hart C, Hogg J, Orborn D, Johnson S, Howard LM 2014, ‘Domestic and sexual violence against patients with severe mental illness’, Psychological Medicine, no. 45, pp. 875-886.
[132] National Domestic and Family Violence Bench Book 2018, Dynamics of domestic and family violence: factors affecting risk, p. 5.
[133] Howard J 2011, Adolescent violence in the home: the missing link in family violence prevention and response, Australian Domestic & Family Violence Clearinghouse, p 1.
[134] Australian Institute of Family Studies 2012, Sibling sexual abuse, ACSSA research summary no. 3, AIFS, Melbourne.
[135] This section refers to cisgender males.
[136] Diemer K 2015, ABS Personal Safety Survey: additional analysis on relationship and sex of perpetrator, documents and working papers, research on violence against women and children, University of Melbourne.
[137] This section refers to cisgender females.
[138] Kertesz M et al. 2020, Women who use force: final report – vol. 1, University of Melbourne, Melbourne, p. 2.
[139] Ibid.
[140] Ibid.
[141] Women’s Legal Service 2018, Policy paper 1: ‘Officer she’s psychotic and I need protection’ – Police misidentification of the ‘primary aggressor’ in family violence incidents in Victoria, p. 1.
[142] Tangney JP, Stuewig J and Hafex L 2011, ‘Shame, guilt and remorse: implications for offender populations’, Journal of Forensic Psychiatry and Psychology, vol. 22, no. 5, pp. 706-723.
[143] Furukawa E et al. 2012, ‘Cross-cultural continuities and discontinuities in shame, guilt, and pride: a study of children residing in Japan, Korea and the USA’, Self & Identity, vol. 11, no. 1, pp. 90-113; Proeve M and Howells K 2002, ‘Shame and guilt in child sexual offenders’, International journal of offender therapy and comparative criminology, vol. 46, no. 6, pp. 657-667.
[144] Loeffler CH, Prelog AJ, Prabha UN andPogrebin MR 2010, ‘Evaluating shame transformation in group treatment of domestic violence offenders’, International Journal of Offender Therapy and Comparative Criminology, vol. 54, no. 4, pp. 517-536.
[145] These common risk factors are also present for child and adult victim survivors, however, the drivers of suicide risk for victims is different to drivers for perpetrators and young people using violence.
[146] MacIsaac et al. 2018, ‘Prevalence and characteristics of interpersonal violence in people dying from suicide in Victoria, Australia’, Asia Pacific Journal of Health, p. 3.
[147] Australian Institute of Criminology 2008, Murder-suicide in Australia, crime facts info no. 176, Australian Institute of Criminology, Canberra.
[148] Cheng P and Jaffe P 2019, ‘Examining depression among perpetrators of intimate partner homicide’, Journal of Interpersonal Violence, doi.org/10.1177/0886260519867151.
[149] Commissioner for Children and Young People 2019, Lost, not forgotten: inquiry into children who died by suicide and were known to Child Protection, Melbourne, p 14.
[150] Ibid., p 14.
[151] Ibid., p. 64.
[152] Ibid.
[153] Ibid., p. 17.
[154] Ibid.
[155] Fowler JC 2012, ‘Suicide risk assessment in clinical practice: pragmatic guidelines for imperfect assessments’, Psychotherapy (Chic), vol. 49, no. 1, pp. 81-90.
[156] Ellis TE, Rufino KA, Allen JG, Fowler JC and Jobes DA 2015, ‘Impact of a suicide-specific intervention within inpatient psychiatric care: the collaborative assessment and management of suicidality’, Suicide and Life-Threatening Behavior, vol. 45, no. 5, pp. 556-566.
[157] Zara C, Weiss C and Parkinson D 2013, Men on Black Saturday: risks and opportunities for change, Women’s Health Goulburn North East.
[158] Ibid.
[159] Expert Advisory Committee on Perpetrator Interventions 2018, Final report, p. 66.
[160] Ibid.
[161] Ibid, p 76.
[162] Judicial College of Victoria 2016, Disability access bench book.
[163] Prevalence among victim survivors often resulted in acquired brain injury as a direct result of the perpetrator’s violence. Prevalence of ABI among victim survivors is reflected above in Section 12.1.9and across the victim survivor–focused practice guides, including through screening questions in intermediate risk assessment about harm including loss of consciousness and hits to the head or neck.
[164] Brain Injury Australia 2018, The prevalence of acquired brain injury among victims and perpetrators of family violence, p vii.
[165] Ibid.
[166] Australian Institute of Health and Welfare 2014, National community services data dictionary, AIHW, Canberra.
[167] State of Victoria 2016, Royal Commission into Family Violence: Summary and recommendations, Parl Paper No 132 (2014–16), Volume IV Report and recommendations, pp. 179, 198, 280.
[168] The term ‘disabling environments’ reflects the social model of disability, which recognises disability is not just a person’s condition but the result of disabling social structures, attitudes and environments; Women with Disabilities Victoria 2014, Position statement: violence against women with disabilities.
[169] Deloitte 2019, Evaluation of new community-based perpetrator interventions and case management trials: final evaluation report, p. 26.
[170] Expert Advisory Committee on Perpetrator Interventions 2018, Final report, p. 71.
[171] It is important to undertake further identification or assessment of family violence behaviours to ensure they are present. A cognitive disability may be present at the same time as family violence behaviours.
[172] Organisations including Synapse, Brain Injury Australia, Scope Australia and the Office of the Public Advocate (who coordinate the Independent Third Persons Program) can provide information about a range of cognitive disabilities and support to consider a tailored approach to interventions, providing adjustments and communication supports.
[173] Expert Advisory Committee on Perpetrator Interventions 2018, Final report, p. 67.
[174] Coghlan S and Millsteed M 2017, Identifying the differences between generalist and specialist family violence perpetrators: risk factors and perpetrator characteristics, In Brief No. 8, Crime Statistics Agency.
[175] Andrews DA 2015, The psychology of criminal conduct, Routledge, Oxfordshire and New York; Mazerolle P et al. 2000, ‘Onset age, persistence, and offending versatility: comparisons across gender’, Criminology vol. 38, no. 4, pp. 1143-1172; Lowenstein J et al. 2016, ‘A systematic review on the relationship between antisocial, borderline and narcissistic personality disorder diagnostic traits and risk of violence to others in a clinical and forensic sample’, Borderline Personality Disorder and Emotion Dysregulation vol. 3, no. 1.
[176] Pollard R and Ferguson C 2020, ‘Intimate partner violence within Australian Defence Force families: an exploratory study’, Journal of Gender-Based Violence, vol. 4, no. 2, p. 4.
[177] Ibid., p. 4.
[178] This can include perpetration of family violence behaviours byproxy
[179] Ibid., p. 17.
[180] Kwan J, Sparrow K, Facer-Irwin E, Thandi G, Fear NT and MacManus D 2020, ‘Prevalence of intimate partner violence perpetration among military populations: a systematic review and meta-analysis’, Aggression and Violence Behavior, vol. 53, art. no. 101419; Saunders DG, Prost SG and Oehme K 2016, ‘Responses of police officers to cases of officer domestic violence: effects and demographic and professional factors’, Journal of Family Violence, vol. 31, pp. 771-784.
[181] Ibid., p. 21.
[182] This guidance uses the term ‘predominant aggressor’ rather than ‘primary aggressor’. This is to avoid mutualising family violence perpetration with use of force and other self-protective behaviours that can lead to misidentification of the ‘real’ perpetrator.
[183] Women’sLegal Service 2018, Policy paper 1: “Officer she’s psychotic and I need protection” – Police misidentification of the ‘primary aggressor’ in family violence incidents in Victoria.
[184] Rainbow Health Victoria 2020, Pride in prevention: a guide to primary prevention of family violence experienced by LGBTIQ communities, p.9.
[185] No to Violence 2019, Discussion paper: predominant aggressor identification and victim misidentification, No to Violence, Melbourne.
[186] Larance LY, Goodmark L, Miller SL and Dasgupta SD 2018, ‘Understanding and addressing women’s use of force in intimate relationships: a retrospective’, Violence Against Women, vol. 25, no. 1, pp. 56-80.
[187] Kertesz M 2020, Women who use force: final report – vol. 1, University of Melbourne, Melbourne.
[188] Victoria Police Manual, Family Violence, ‘Identifying the primary aggressor’, pp. 12-13, last updated 19 February 2021.
[189] Evidence on this item is based on cisgender heterosexual relationships. Evidence is not present for how this should inform predominant aggressor identification in LGBTIQ relationships.
[190] EACPI 2019, Final report, State Government of Victoria, Melbourne, p. 22.
[191] Adapted from State Government of Western Australia 2015, Western Australian Family and Domestic Violence Common Risk Assessment and Risk Management Framework, 2nd ed.
[192] No to Violence 2020, NSW risk, safety and support framework, No to Violence, Melbourne.
[193] RMIT Centre for Innovative Justice 2019, Foundations for family and domestic violence perpetrator intervention systems, RMIT CIJ, p. 8.
[194] State of Victoria 2008, Strong Culture, Strong Peoples, Strong Families: Towards a safer future for Indigenous families and communities — 10 year plan, 2nd ed.
[195] Adapted from Merriam-Webster dictionary definition of intersectionality.
[196] Refer to George v Rockett, 1990, 170 CLR 104.